In the bustling theater of modern medicine, few stars have risen with the dazzling speed and intensity of GLP-1 receptor agonists. Brands like Ozempic, Wegovy, Mounjaro, and Zepbound have become household names, whispered in doctor’s offices, debated on social media, and celebrated in countless testimonials. They arrived like a seismic shift, promising not just modest weight loss, but a major transformation, a definitive answer to the intractable challenge of obesity that has plagued millions for decades. The narrative, often amplified by headlines and viral stories, paints a picture of liberation: inject a small dose, shed significant pounds, and reclaim a healthier life.
Yet, as with any phenomenon that captivates the collective imagination, a closer look beyond the initial shimmer reveals a more complex landscape. The clinical trials that launched these medications into orbit undeniably demonstrated impressive average weight loss percentages, igniting a fervent hope that this was finally the magic bullet. But what happens when these powerful drugs leave the controlled environment of a trial and enter the chaotic, unpredictable realm of everyday life? When the ideal patient selection, strict adherence protocols, and constant medical supervision of research settings give way to the myriad variables of individual biology, lifestyle, access, and personal discipline?
The story of GLP-1s is still unfolding, but real-world data, collected from the lived experiences of millions, is beginning to paint a different, more nuanced picture. It’s a narrative not of universal, guaranteed major weight loss for all, but of significant potential tempered by profound variability, persistent challenges, and the undeniable truth that even the most revolutionary pharmaceutical tools are just that – tools, not standalone solutions. For a knowledgeable audience, accustomed to dissecting data and understanding biological complexity, it’s time to move beyond the sensational and delve into the granular realities of GLP-1s in practice.
The Siren Song of the Syringe: Understanding the Promise
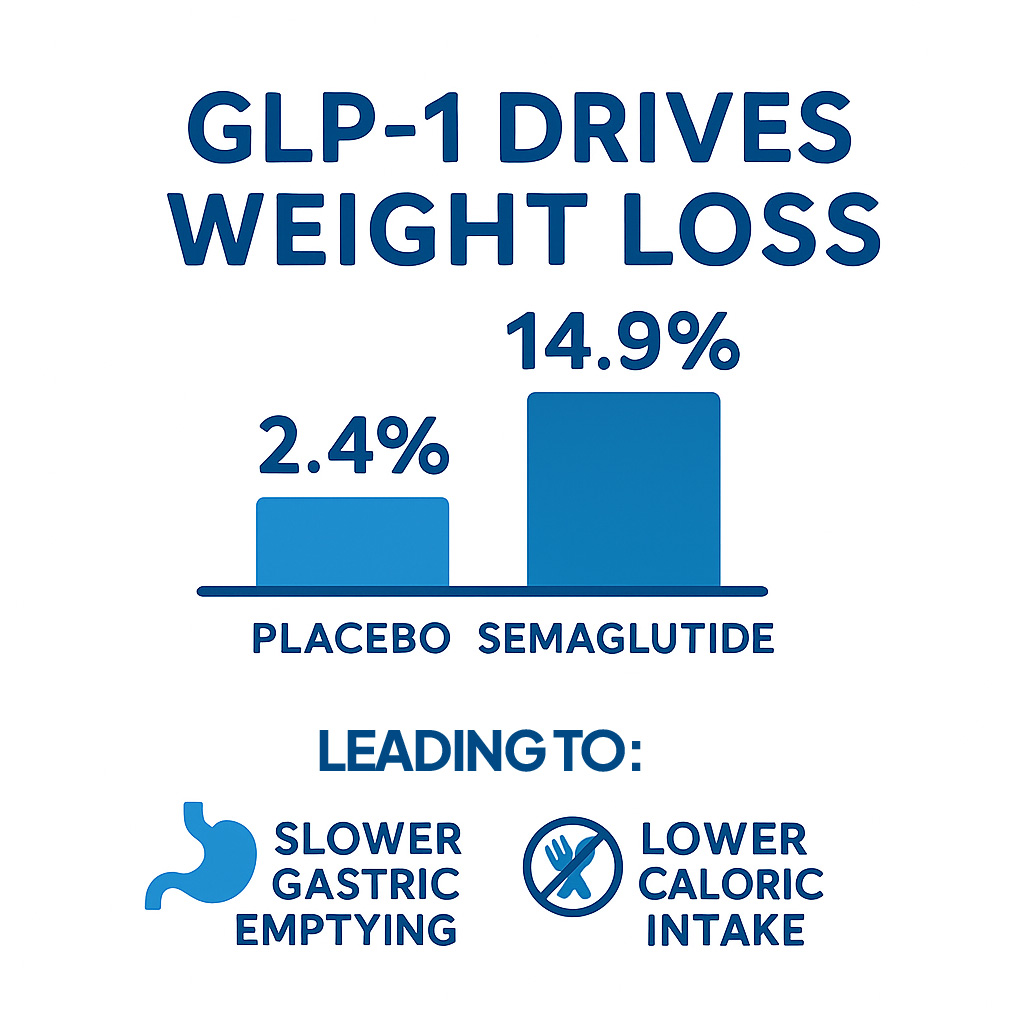
Before we dissect the real-world experience, it’s crucial to understand why GLP-1s created such a powerful ripple. Glucagon-like peptide-1 is a naturally occurring hormone produced in the gut, released in response to food intake. It plays several critical roles: stimulating insulin secretion, suppressing glucagon release, slowing gastric emptying, and acting on the brain to reduce appetite and increase feelings of fullness. These mechanisms collectively lead to reduced food intake and, subsequently, weight loss.
The pharmaceutical versions of GLP-1s are designed to mimic and amplify these natural effects. Early formulations, like liraglutide, showed promising but modest weight loss. The true game-changers emerged with semaglutide (Wegovy for weight loss, Ozempic for diabetes with off-label weight loss use) and tirzepatide (Zepbound for weight loss, Mounjaro for diabetes), which also acts on GIP (glucose-dependent insulinotropic polypeptide) receptors, offering an even more potent metabolic punch.
The pivotal clinical trials – the STEP trials for semaglutide and the SURMOUNT trials for tirzepatide – delivered unprecedented results. Participants on the highest doses of semaglutide achieved an average of 15-17% total body weight loss, while tirzepatide pushed this further, reaching an average of 20-22% weight loss. These figures represented a paradigm shift. For individuals struggling with obesity, who had often seen only marginal success with diet and exercise alone, and whose only other effective option was bariatric surgery, these drugs felt like a revelation. The promise was clear: significant, sustained weight loss, delivered through a weekly or daily injection, without the invasiveness of surgery. The media, understandably, latched onto these impressive averages, often translating them into a simple, compelling narrative: "major weight loss guaranteed."
From Lab Bench to Living Room: The Real-World Unveiling
The transition from controlled clinical trials to the vast, heterogeneous landscape of real-world application inevitably introduces complexities. In a trial, participants are carefully selected, often highly motivated, and receive intensive support, including regular counseling on diet and exercise. Adherence is meticulously tracked, and side effects are closely monitored and managed. In the "real world," these conditions rarely hold true.
As millions of prescriptions have been filled, a more nuanced understanding of GLP-1 effectiveness has emerged, highlighting significant variability in individual responses. The "average" weight loss reported in trials, while statistically robust, does not predict the experience of every single patient.
The Spectrum of Success: Variability is the Rule, Not the Exception
One of the most striking revelations from real-world data is the sheer variability in individual responses to GLP-1s. While some individuals mirror or even exceed the impressive weight loss seen in clinical trials, a significant proportion experience more modest results, or even struggle to lose weight at all.
This variability isn’t surprising to those familiar with pharmacogenomics and the intricate biology of weight regulation. Our bodies are not uniform machines; they are complex biological systems influenced by a myriad of factors. Genetics play a substantial role. Polymorphisms in genes related to GLP-1 receptor sensitivity, appetite regulation, and metabolic rate can influence how an individual responds to the medication. Some people are simply "better responders" due to their unique genetic makeup.
Beyond genetics, baseline metabolic status is critical. Individuals with higher initial body mass indexes (BMIs) and more severe metabolic dysfunction sometimes show more dramatic initial weight loss, partly because they have more weight to lose and partly due to the profound impact of the drugs on their dysregulated systems. Conversely, those closer to a "healthy" weight or with less severe metabolic issues might see less dramatic, albeit still clinically meaningful, changes.
Adherence is another major factor. While clinical trials boast high adherence rates, real-world data often shows a drop-off. Missing doses, inconsistent administration, or discontinuing the medication prematurely due to side effects, cost, or perceived lack of efficacy all contribute to attenuated results. The "average" weight loss from trials assumes consistent, optimal use, a standard often difficult to maintain in daily life.
Furthermore, the "real-world" often means less structured dietary and exercise intervention. While GLP-1s reduce appetite, they don’t dictate food choices. An individual who continues to make poor dietary decisions, even if consuming less overall, may not achieve the same metabolic benefits or weight loss as someone who pairs the medication with conscious, healthier food choices and increased physical activity. The drug acts as an appetite suppressant and a metabolic modulator, but it cannot override every lifestyle choice.
The Unavoidable Plateau: When Progress Stalls
Another common theme emerging from real-world observations is the plateau effect. For many individuals, weight loss is initially rapid and encouraging, but then slows down significantly or stops altogether, even while consistently taking the medication. This phenomenon, often frustrating for patients, is well-documented in obesity research and is a testament to the body’s powerful homeostatic mechanisms.
As an individual loses weight, the body often perceives this as a threat to its established energy reserves. It responds by implementing various adaptive mechanisms to resist further loss. Resting metabolic rate can decrease, meaning fewer calories are burned at rest. Hormonal signals related to appetite and satiety can shift, potentially counteracting some of the drug’s effects. Ghrelin, the hunger hormone, might increase, while leptin, the satiety hormone, might decrease. The body essentially "fights back" to maintain its current weight, or even regain lost weight.
This metabolic adaptation means that the dose that was initially effective might become less so over time. While dose escalation (e.g., from 0.25mg to 2.0mg for semaglutide) is part of the treatment protocol, even at maximal doses, many individuals will experience a plateau. Understanding this is crucial for managing patient expectations and avoiding the demoralization that can lead to discontinuation. It underscores that weight loss is not a linear journey, and the body’s internal thermostat for weight is stubbornly resistant to change.
The Shadow of Regain: What Happens When You Stop?
Perhaps the most critical, yet often overlooked, aspect of GLP-1s in the context of "guaranteed major weight loss" is the issue of weight regain upon discontinuation. The vast majority of clinical trial data indicates that once GLP-1 medication is stopped, weight regain is common, often significant, and can return individuals close to their starting weight within a year or two.
This isn’t a failure of the drug; it’s a fundamental aspect of obesity as a chronic, relapsing disease. GLP-1s manage the symptoms of obesity – excess weight, dysregulated appetite, metabolic dysfunction – much like insulin manages diabetes or statins manage high cholesterol. They do not "cure" the underlying condition. When the medication is withdrawn, the physiological mechanisms that were being suppressed or modulated revert to their pre-treatment state. Appetite returns to baseline (or even increases due to compensatory mechanisms), satiety signals weaken, and the body’s propensity to store fat reasserts itself.
This reality carries profound implications for treatment paradigms. It strongly suggests that GLP-1s, for many, need to be considered a long-term, potentially lifelong, treatment for obesity. This shifts the narrative from a "fix" to a "management strategy," similar to other chronic diseases. This long-term perspective introduces new considerations regarding cost, access, potential long-term side effects, and the psychological burden of continuous medication. The promise of "major weight loss" often implies a finite journey; the reality is often an ongoing commitment.
Beyond the Needle: The Indispensable Role of Lifestyle
While GLP-1s are powerful tools, real-world experience reinforces a timeless truth: lifestyle factors remain paramount. The drugs are not a substitute for healthy eating and regular physical activity; rather, they are designed to facilitate these changes by making it easier for individuals to adhere to them.
Many patients report that GLP-1s "quiet the food noise" – the constant intrusive thoughts about food, cravings, and insatiable hunger. This reduction in hedonic eating and primal urges creates a window of opportunity. However, whether an individual seizes that opportunity to adopt sustainable, healthy habits dictates the long-term success and quality of their weight loss.
Those who pair their GLP-1 medication with mindful eating, a balanced diet rich in protein and fiber, adequate hydration, and consistent exercise routines not only tend to lose more weight but also maintain it more effectively. They experience better body composition changes (losing fat while preserving muscle mass) and achieve superior metabolic health outcomes. Conversely, individuals who rely solely on the medication without addressing underlying dietary patterns or physical inactivity may see diminished results, experience more muscle loss, and be more susceptible to regain.
The narrative of GLP-1s as "effortless" weight loss is misleading. While they reduce the struggle, they don’t eliminate the need for effort. They empower individuals to make healthier choices, but the choices themselves still need to be made. This collaborative approach – medication working in concert with lifestyle modification – is where the true, sustainable benefits of GLP-1s are realized.