The human body is a marvel of biological engineering, undergoing incredible transformations from conception to old age. Among these changes, few provoke as much curiosity, anxiety, and myth-making as the development of the male reproductive organ: the penis. From the earliest whispers of its formation in the womb to its final, mature state and the subtle shifts that come with aging, the journey of penile growth is a complex, hormonally orchestrated symphony. This is the story of that growth, a narrative spanning decades, shaped by genetics, hormones, and the inexorable march of time.
Chapter 1: The Blueprint – Penile Genesis in the Womb
Our story begins not in adolescence, but in the earliest, most delicate stages of life: within the womb. The formation of the penis is a testament to the intricate dance of genetics and embryology, a process that lays the fundamental blueprint for what is to come.
Around the fifth to sixth week of gestation, an embryo possesses a remarkable bipotentiality. At this stage, the external genitalia are undifferentiated, meaning they have the capacity to develop into either male or female structures. This indifferent stage is characterized by the presence of a genital tubercle, urethral folds, and labioscrotal swellings – the raw materials from which a penis or clitoris will eventually emerge.
The critical turning point arrives with the presence, or absence, of the Y chromosome. If a Y chromosome is present, a specific gene called SRY (Sex-determining Region Y) springs into action around week 7. This gene acts as the master switch, initiating the cascade of events that leads to male sexual differentiation. The SRY gene triggers the development of testes from the undifferentiated gonads. Once formed, these embryonic testes become the primary architects of male development, producing a crucial hormone: testosterone.
Testosterone, however, is often not the direct agent for external genital masculinization. Instead, it serves as a precursor. Within the target cells of the genital tubercle and surrounding tissues, an enzyme called 5-alpha-reductase converts testosterone into its more potent derivative, dihydrotestosterone (DHT). It is DHT that drives the transformation of the indifferent external genitalia. Under the influence of DHT, the genital tubercle elongates and develops into the glans and shaft of the penis. The urethral folds fuse along the ventral surface, enclosing the urethra within the developing penile shaft, and the labioscrotal swellings fuse to form the scrotum.
This period, roughly from weeks 7 to 12, is a time of incredibly rapid and precise growth. By the end of the first trimester, the basic structure of the penis is largely established. At birth, a full-term male infant typically has a stretched penile length ranging from 2.8 to 4.2 centimeters (approximately 1.1 to 1.7 inches). This initial length is a direct result of the intense hormonal activity during fetal development, a "first growth spurt" orchestrated entirely within the protective confines of the uterus. Any significant disruption to this delicate hormonal balance or genetic programming during this critical window can lead to congenital anomalies, such as micropenis (an abnormally small penis) or hypospadias (where the urethral opening is not at the tip of the penis). Thus, the story of penile growth begins long before birth, a testament to the profound impact of our earliest developmental chapters.
Chapter 2: The Quiet Years – Infancy and Childhood
Following the dramatic architectural achievements in the womb, the penis embarks on a period of relative calm, a phase often characterized by minimal and almost imperceptible growth. This chapter spans infancy and the entirety of childhood, a time when the body is busy with other developmental priorities.
The very first year of life, however, offers a brief echo of the hormonal activity seen in utero. This period is sometimes referred to as "mini-puberty of infancy." Shortly after birth, the male infant experiences a transient surge in gonadotropin (LH and FSH) and testosterone levels, driven by the lingering influence of maternal hormones and the initial awakening of the infant’s own hypothalamic-pituitary-gonadal (HPG) axis. This neonatal testosterone surge can lead to a slight, albeit temporary, increase in penile length and testicular volume. It’s a subtle flourish before the main act, a final hormonal hurrah that helps to "masculinize" the brain and other tissues further.
But just as quickly as it appears, this mini-puberty subsides. By six months to a year of age, the HPG axis, the master control system for sexual development, goes largely dormant. It enters a state of deep slumber, often referred to as the "juvenile pause." During this extensive period, which lasts throughout childhood, the levels of sex hormones – testosterone in particular – are extremely low. Consequently, penile growth is minimal.
From toddlerhood through the pre-teen years, the penis remains relatively small and inconspicuous compared to its eventual adult size. While the rest of the child’s body undergoes steady growth in height, weight, and muscle mass, the penis grows at a much slower rate, roughly proportional to overall body growth, rather than experiencing dedicated, accelerated development. This can sometimes be a source of anxiety for parents, who may compare their child’s anatomy to others or to their own memories of adolescence. However, this small size is entirely normal and expected during childhood. It’s a physiological holding pattern, a period of quiet maturation where the body is conserving its resources for the explosive changes that lie ahead.
The HPG axis is not entirely inactive during this time; it is merely exquisitely sensitive to negative feedback, meaning even tiny amounts of sex hormones are enough to keep it suppressed. This "sleep mode" ensures that puberty does not commence prematurely, allowing for the full development of other bodily systems before the dramatic onset of sexual maturation. The quiet years are a necessary prelude, a time of patient waiting before the grand awakening that will define the next significant chapter in the penis’s growth story.
Chapter 3: The Grand Awakening – Puberty’s Transformative Power
If fetal development was the blueprint and childhood the quiet interlude, then puberty is undeniably the grand awakening – the most dramatic and rapid period of penile growth. This transformative phase marks the true onset of sexual maturation and is driven by a complex, beautifully orchestrated hormonal cascade.
The signal for puberty to begin originates deep within the brain, in the hypothalamus. After years of dormancy, the hypothalamus begins to secrete pulsatile bursts of gonadotropin-releasing hormone (GnRH). This chemical messenger travels to the pituitary gland, a small but mighty organ located at the base of the brain. In response, the pituitary gland releases two crucial hormones: luteinizing hormone (LH) and follicle-stimulating hormone (FSH). These gonadotropins, as they are known, then journey through the bloodstream to their ultimate target: the testes.
Upon reaching the testes, LH stimulates the Leydig cells to produce and secrete large quantities of testosterone, while FSH promotes sperm production and the development of the seminiferous tubules. It is the surge in testosterone that acts as the primary driver of male secondary sexual characteristics, including the rapid growth of the penis.
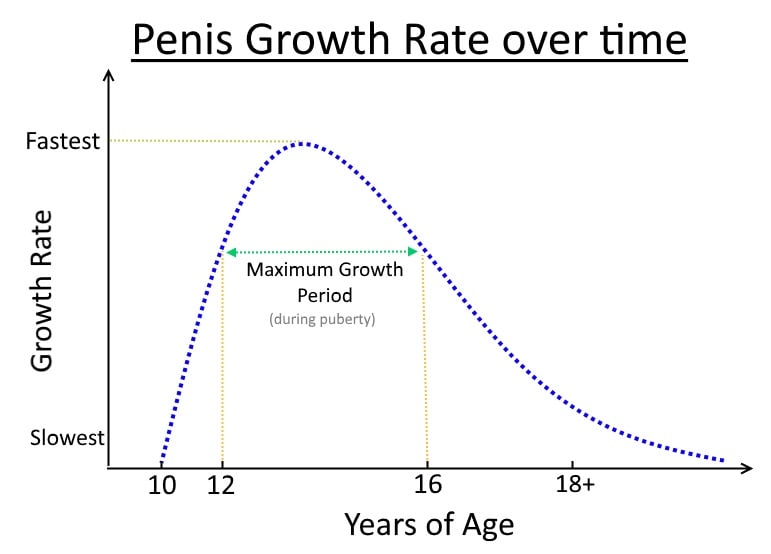
Puberty typically begins between the ages of 9 and 14, though there is significant individual variation. The first clinical sign of male puberty is usually testicular enlargement, often followed by the appearance of pubic hair. Penile growth, both in length and circumference, typically commences a bit later, usually around Tanner Stage 3 of pubertal development, which occurs approximately a year after the initial testicular enlargement.
The mechanism of penile growth during puberty is fascinating. Under the sustained influence of high levels of testosterone (and its conversion to DHT in target penile tissues), the cells within the corpora cavernosa – the two main erectile chambers of the penis – proliferate and enlarge. There’s an increase in smooth muscle cells, collagen fibers, and elastic tissue, contributing to both length and girth. The vascular network also expands and matures, preparing the penis for its eventual erectile function. This growth is not necessarily linear or constant; it can occur in spurts, with periods of rapid expansion followed by slower, more gradual changes.
For the individual experiencing it, this phase is often a mix of excitement, self-consciousness, and intense curiosity. The sudden changes can be startling, prompting comparisons with peers and a heightened awareness of one’s developing body. The "story" here is not just biological but deeply psychological: the negotiation of a new body image, the grappling with newfound sexual feelings, and the often-anxious question of "Am I normal?"
The duration of this pubertal growth spurt varies, but it generally continues for several years. Penile growth usually decelerates towards the end of puberty, typically in the late teens. While the most rapid growth occurs earlier in puberty, some subtle changes and maturation can continue until around 18-21 years of age. Factors influencing the timing and pace of puberty, and thus penile growth, include genetics (a strong determinant), nutrition, overall health, and even geographical location or environmental factors. Malnutrition or chronic illness, for instance, can delay the onset or slow the progression of puberty.
Alongside penile growth, the surge in testosterone also orchestrates a symphony of other pubertal changes: deepening of the voice, growth of facial and body hair, increased muscle mass, changes in body odor, and the development of libido. The penis’s growth is therefore an integral, albeit highly visible, part of a much broader biological transformation, signaling the transition from childhood to reproductive maturity.
Chapter 4: The Plateau – Adulthood and Maturation
With the tempestuous hormonal surges of puberty gradually subsiding, the penis enters a new chapter: adulthood. This is the stage of maturation and stabilization, where growth largely ceases, and the organ reaches its final, mature size.
So, when exactly does the penis stop growing? While the most dramatic changes conclude by the late teens, it’s generally accepted that penile growth, both in length and girth, ceases by the early twenties, typically between 18 and 21 years of age. By this point, the hormonal environment has stabilized, and the target cells in the penile tissues have largely completed their proliferation and differentiation in response to pubertal testosterone levels. The growth plates in the bones have fused, and the body has reached its full adult stature; similarly, the penis reaches its structural maturity.
The cessation of growth is a complex process. It involves a combination of factors: the downregulation of androgen receptors in penile tissues, the establishment of negative feedback loops that regulate hormone production, and the structural limits of tissue expansion. Once these processes are complete, further significant growth is no longer physiologically possible under normal circumstances.
This brings us to the often-discussed topic of "normal" size. It’s crucial to understand that there is a wide range of normal penile dimensions. Studies consistently show an average erect length of approximately 5.1 to 6.3 inches (13 to 16 centimeters) and an average flaccid length of about 3.6 inches (9.16 centimeters). However, these are just averages, and healthy penises exist comfortably outside these figures. Genetics play a paramount role in determining an individual’s final size, just as they dictate height, hair color, or shoe size. While ethnicity can sometimes be associated with slight variations, it’s far less influential than individual genetic makeup, and considerable overlap exists across all populations.
Despite the scientific consensus on the normal range and the factors influencing size, societal pressures and myths continue to fuel anxiety. Misinformation abounds, with unsubstantiated claims about special diets, exercises, or supplements that can supposedly increase penile size after puberty. It is important to emphasize that once the growth plates of the penis have fused and hormonal development is complete, these methods are ineffective and can even be harmful. The final size achieved in early adulthood is, for the vast majority of individuals, the size they will maintain.
This chapter in the penis’s story is also profoundly psychological. For many, reaching adulthood involves coming to terms with their body, including their penis. Self-acceptance, understanding the wide spectrum of normal, and recognizing that function and intimacy are far more important than mere dimensions, are key aspects of a healthy relationship with one’s body. While medical conditions like micropenis (a congenital condition where the penis is significantly smaller than average) or Peyronie’s disease (an acquired condition causing penile curvature and sometimes shortening due to scar tissue) exist as exceptions, they are distinct from the typical developmental trajectory and require specific medical attention. For most men, adulthood represents the plateau of penile development, a stable state of maturity.



