For decades, it has stood as an unassailable arbiter of health, a simple numerical shorthand whispered in doctor’s offices, plastered across fitness articles, and even tattooed onto the collective consciousness as a measure of societal well-being: the Body Mass Index, or BMI. Calculated with disarming simplicity from just two variables—your weight and your height—it has offered a quick, convenient, and seemingly universal gauge of whether you fall into the categories of underweight, normal, overweight, or obese. But beneath its veneer of scientific authority, a growing chorus of medical professionals, researchers, and increasingly, the public, are questioning its dominion. The story of BMI is one of an expedient tool that outlived its original intent, a blunt instrument in a world demanding precision. Its reign, while long and influential, is finally giving way to a more nuanced, insightful, and ultimately, more accurate understanding of what truly constitutes a healthy body: the Waist-to-Hip Ratio (WHR).
This isn’t merely a semantic debate about metrics; it’s a fundamental shift in how we perceive the silent, internal drama of our own physiology. It’s a journey from focusing on the mere quantity of mass to understanding the critical quality and distribution of that mass. And in this evolving narrative of health assessment, the WHR emerges as a compelling protagonist, offering a clearer window into our metabolic destiny than its venerable, but increasingly anachronistic, predecessor.
The Reign of BMI: A Historical Context and Its Unveiling Limitations
To understand why BMI is losing its luster, we must first appreciate its origins and the context in which it rose to prominence. The story begins not in a modern clinic, but in the 19th century, with a Belgian astronomer, mathematician, and statistician named Adolphe Quetelet. In the 1830s, Quetelet developed what he called the "Quetelet Index" as a quick and easy way to statistically measure the obesity of the general population to classify populations, not individuals. His aim was to describe the "l’homme moyen" – the average man – and track population health trends, not to diagnose or assess individual health risks. It was never intended to be a clinical diagnostic tool for a single person.
Fast forward to the mid-20th century, and the Quetelet Index found a new champion in American physiologist Ancel Keys. Keys, renowned for his studies on diet and heart disease, renamed it the Body Mass Index (BMI) in 1972 and championed its use in epidemiological studies. Its simplicity was its strength: requiring only height and weight, it was non-invasive, inexpensive, and easy to calculate for large populations. Public health organizations, insurance companies, and even governmental bodies eagerly adopted it. It offered a standardized way to categorize individuals, set policy, and quantify the burgeoning global obesity epidemic. For decades, it served as a convenient benchmark, its classifications becoming almost sacrosanct: a BMI below 18.5 was underweight, 18.5-24.9 was normal, 25-29.9 was overweight, and 30 or above was obese.
However, despite its widespread adoption and apparent utility, the cracks in the BMI’s foundation began to show almost immediately, widening into gaping chasms as our understanding of human physiology deepened.
1. The Body Composition Blind Spot: Muscle vs. Fat
The most glaring limitation of BMI is its inability to differentiate between lean muscle mass and fat mass. This is the classic "bodybuilder paradox." Imagine a professional athlete—a rugby player, a weightlifter, or a bodybuilder—who is incredibly muscular, lean, and physically fit. Due to their high muscle mass, they are often classified as "overweight" or even "obese" by BMI standards. Their density, born of strength and discipline, pegs them into a risk category that clearly doesn’t apply. Conversely, an individual with a low muscle mass and a higher proportion of fat, often referred to as "skinny fat" or "TOFI" (Thin Outside, Fat Inside), might fall within the "normal" BMI range, yet be at significant metabolic risk. The BMI simply treats all weight the same, disregarding the crucial qualitative difference between muscle and fat.
2. The Fat Distribution Blind Spot: Where the Fat Sits Matters More
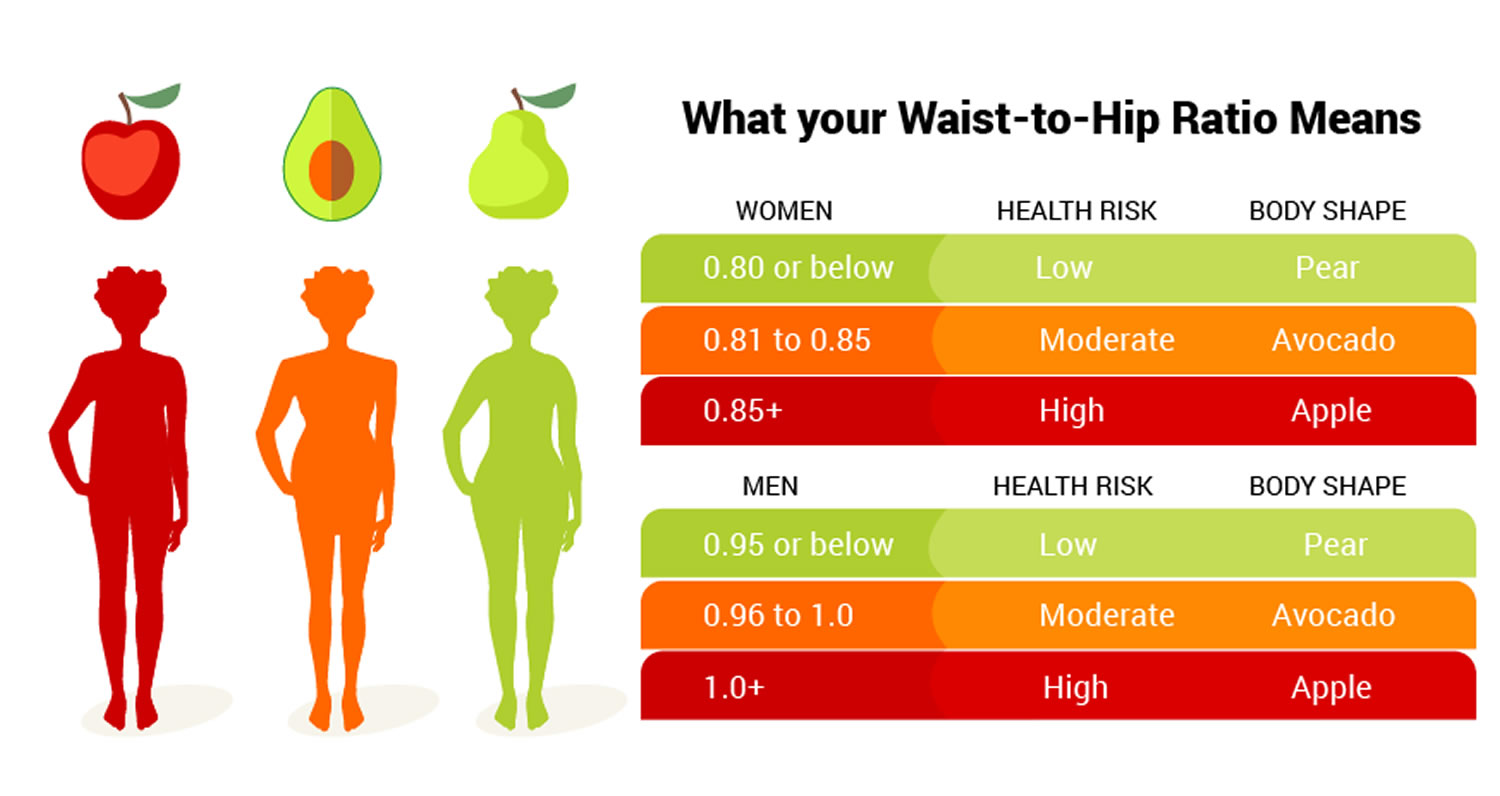
Perhaps the most critical oversight of BMI, and the one that directly paves the way for the superiority of WHR, is its complete indifference to where fat is stored in the body. Two individuals with the exact same BMI could have vastly different body shapes and, critically, vastly different health risks. One might carry their weight predominantly in their hips and thighs (a "pear" shape), while the other might store it around their abdomen (an "apple" shape). BMI sees them as identical, yet their internal metabolic landscapes are poles apart. This is where the narrative truly shifts, moving beyond the superficial numbers to the profound implications of anatomical geography.
3. Age, Sex, and Ethnicity: One Size Does Not Fit All
BMI thresholds, largely derived from Caucasian populations, fail to adequately account for the natural variations across different demographics. As we age, for instance, body composition naturally shifts, with a tendency to lose muscle mass and gain fat, particularly visceral fat. A BMI of 25 in a 20-year-old might carry different implications than the same BMI in a 70-year-old. Similarly, men and women naturally distribute fat differently due to hormonal influences. Women tend to have higher overall body fat percentages and store more fat in their hips and thighs, especially pre-menopause.
Furthermore, ethnic variations are significant. Studies have shown that Asian populations, for example, may face increased health risks at lower BMIs compared to Caucasians, while some Polynesian populations naturally have higher muscle mass and bone density, making standard BMI thresholds misleading. To apply a single, universal metric to such a diverse tapestry of human physiology is to ignore fundamental biological realities.
4. The "Healthy Obese" and "TOFI" Paradoxes
The limitations of BMI have given rise to two particularly unsettling paradoxes. The "healthy obese" are individuals who, despite having a BMI in the obese range, exhibit no signs of metabolic dysfunction (normal blood pressure, cholesterol, blood sugar, and insulin sensitivity). While this group’s long-term health trajectory is still debated, their existence undeniably challenges the blanket condemnations of high BMI. Conversely, the "TOFI" (Thin Outside, Fat Inside) individuals, with a "normal" BMI, can harbor significant amounts of visceral fat, leading to insulin resistance, inflammation, and an elevated risk for metabolic diseases. These real-world scenarios highlight BMI’s fundamental flaw: it is an indicator of weight relative to height, not health relative to metabolic risk.
Unveiling the Superior Metric: The Waist-to-Hip Ratio (WHR)
The growing awareness of BMI’s shortcomings has driven a scientific quest for a more accurate, nuanced, and predictive measure of health risk. The answer, it turns out, lies not in a new, complex biomarker, but in a simple ratio that directly addresses BMI’s biggest blind spot: the Waist-to-Hip Ratio (WHR). This metric shifts our focus from the sheer volume of body mass to the critical question of where that mass is distributed, particularly how much is concentrated around the abdomen.
The "aha!" moment in this evolving narrative came with the understanding that not all fat is created equal. There are broadly two types of fat that concern us:
- Subcutaneous Fat: This is the fat stored just beneath the skin, the jiggly fat you can pinch. While excessive amounts can contribute to overall weight and carry some health implications, it is generally considered less metabolically active and less dangerous than its deeper counterpart.
- Visceral Fat: This is the deeply embedded fat that surrounds your internal organs in the abdominal cavity. This is the truly insidious fat, the silent actor in a metabolic drama that can lead to chronic disease.
Understanding the Menace of Visceral Fat
Visceral fat is not merely an inert storage depot; it is an active endocrine organ, a miniature factory pumping out a cocktail of hormones and inflammatory substances directly into your bloodstream and to your portal vein, which carries blood straight to your liver. This direct line of communication with vital organs makes it particularly dangerous.
- Inflammation: Visceral fat releases pro-inflammatory cytokines (e.g., TNF-alpha, IL-6), which contribute to systemic inflammation, a known driver of numerous chronic diseases, including heart disease, diabetes, and certain cancers.
- Insulin Resistance: It releases free fatty acids into the liver, disrupting its ability to regulate blood sugar effectively. This can lead to insulin resistance, a precursor to type 2 diabetes.
- Hormonal Disruption: Visceral fat can interfere with the body’s hormonal balance, affecting everything from appetite regulation to reproductive hormones.
- Cardiovascular Impact: It directly contributes to elevated blood pressure, unhealthy cholesterol profiles (high LDL, low HDL), and increased risk of atherosclerosis (hardening of the arteries), significantly raising the risk of heart attacks and strokes.




