In the quiet corridors of women’s health, a condition often whispers rather than shouts. It’s a profound, pervasive reality for millions, yet frequently remains shrouded in silence, dismissed as an inevitable consequence of aging, or simply too embarrassing to discuss. This is the story of atrophic vaginitis, more commonly known as vaginal atrophy – a narrative woven from the threads of biology, discomfort, emotional struggle, and ultimately, the triumph of knowledge and self-advocacy.
To understand atrophic vaginitis is to understand the intricate dance of hormones within the female body, particularly estrogen. It’s a journey into the delicate ecosystem of the vagina and the profound impact its health has on a woman’s overall well-being, intimacy, and sense of self. Far from a trivial complaint, vaginal atrophy is a chronic, progressive condition that, left unaddressed, can significantly diminish quality of life. For the knowledgeable audience, we delve deep into its etiology, manifestation, diagnosis, and the comprehensive landscape of modern therapeutic approaches.
The Estrogen Symphony: A Foundation for Understanding
At the heart of vaginal atrophy lies a fundamental shift in the body’s hormonal composition: a decline in estrogen. Estrogen, often lauded for its role in reproduction and secondary sexual characteristics, is a vital hormone with far-reaching effects throughout the body, including maintaining the health and vitality of the vaginal and vulvar tissues.
Prior to menopause, the ovaries produce a steady supply of estrogen. This estrogen acts as a crucial nutrient for the vaginal lining, or epithelium. It promotes the growth of thick, moist, elastic tissue, rich in glycogen. Glycogen, in turn, is metabolized by beneficial lactobacilli bacteria, which produce lactic acid, maintaining a healthy, acidic vaginal pH (typically 3.5-4.5). This acidic environment is a natural defense mechanism, inhibiting the growth of pathogenic bacteria and yeasts, thereby protecting against infections.
Estrogen also ensures robust blood flow to the vaginal area, contributing to lubrication during sexual arousal and overall tissue health. It maintains the integrity of the collagen and elastin fibers within the vaginal walls, providing strength, elasticity, and the characteristic folds or rugae that allow the vagina to stretch during intercourse and childbirth. The labia majora and minora, the clitoris, and the urethra also rely on adequate estrogen levels for their structure and function.
The Discordant Note: When Estrogen Levels Fall
The decline in estrogen, most notably associated with menopause, strikes a discordant note in this carefully orchestrated symphony. Menopause, defined as 12 consecutive months without a menstrual period, marks the permanent cessation of ovarian function. During the perimenopausal transition and into postmenopause, estrogen production plummets.
However, menopause is not the sole culprit. Several other scenarios can lead to estrogen deficiency and, consequently, atrophic vaginitis:
- Surgical Menopause: Bilateral oophorectomy (surgical removal of both ovaries) immediately halts estrogen production, leading to an abrupt and often severe onset of symptoms.
- Chemotherapy and Radiation Therapy: These cancer treatments can damage the ovaries, inducing premature menopause or temporary ovarian suppression.
- Certain Medications:
- Aromatase Inhibitors: Used in the treatment of estrogen-receptor-positive breast cancer (e.g., anastrozole, letrozole, exemestane) block the conversion of androgens to estrogen, leading to profound estrogen deprivation.
- GnRH Agonists/Antagonists: Used for conditions like endometriosis, uterine fibroids, or prostate cancer (e.g., leuprolide, goserelin) suppress ovarian estrogen production.
- Anti-estrogens: Tamoxifen, also used in breast cancer treatment, can have anti-estrogenic effects on vaginal tissue, although it can also be estrogenic in other tissues.
- Breastfeeding: High prolactin levels during lactation can temporarily suppress ovarian function and estrogen production, often leading to temporary vaginal dryness and atrophy.
- Eating Disorders: Severe caloric restriction and low body fat can disrupt the hypothalamic-pituitary-ovarian axis, leading to amenorrhea and low estrogen.
- Primary Ovarian Insufficiency (POI): When ovaries stop functioning before age 40.
Regardless of the cause, the consequences of sustained low estrogen on the genitourinary tissues are predictable and progressive.
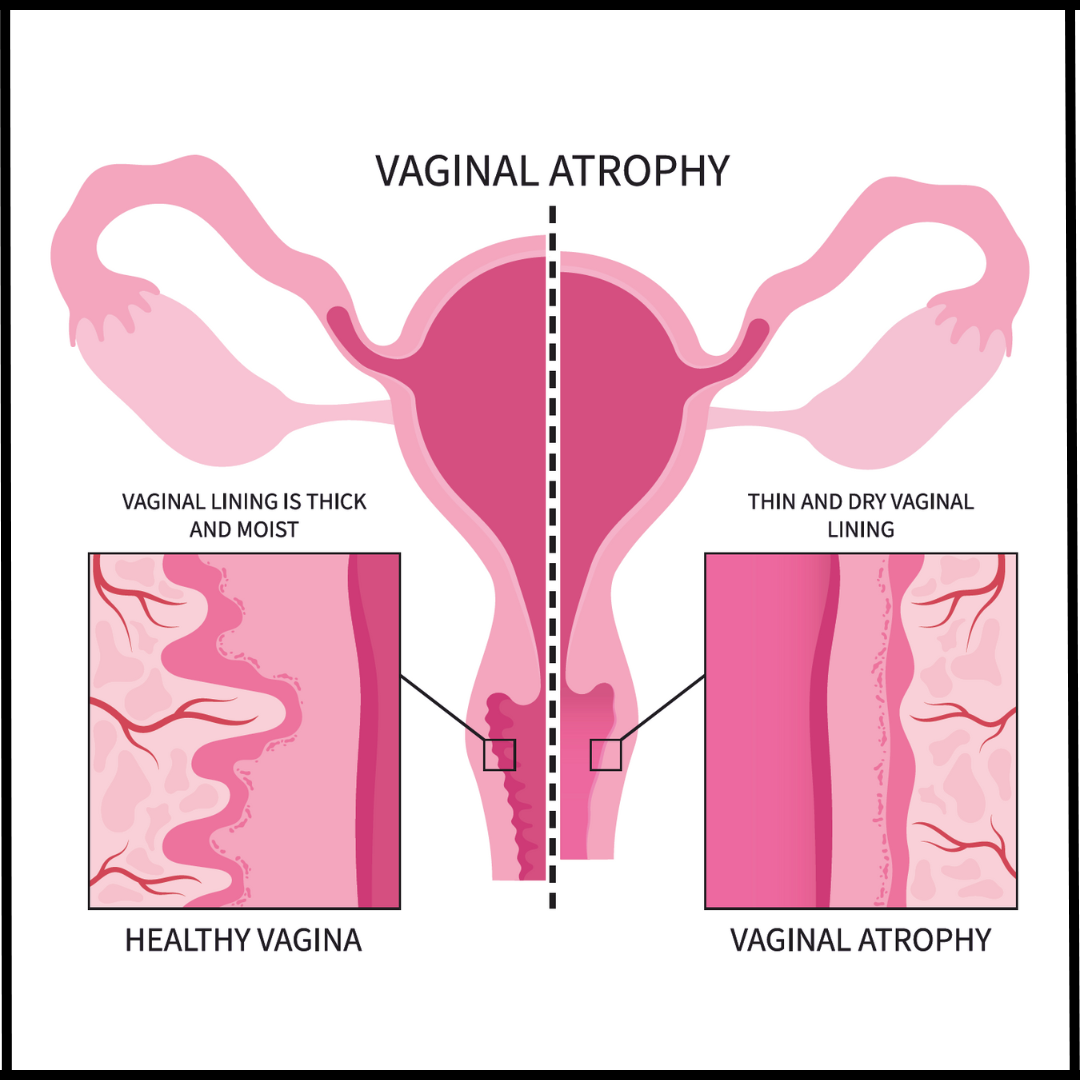
The Transformation: What Happens to the Tissues
With the withdrawal of estrogen, the vibrant, healthy vaginal epithelium undergoes a series of regressive changes:
- Thinning: The multi-layered squamous epithelium thins dramatically, becoming more fragile and delicate.
- Loss of Rugae: The characteristic folds of the vaginal wall flatten, leading to a smoother, less elastic surface.
- Decreased Blood Flow: The rich vascular network diminishes, resulting in paler tissue color and reduced natural lubrication.