The world is a tapestry of individual footsteps, each leaving a unique impression on the path of life. Among these myriad gaits, one stands out for its distinctive inward turn: the pigeon-toed walk. It’s a term often whispered with a mix of concern and curiosity, frequently observed in the tentative steps of a toddler or the confident stride of an older child. But what does it truly mean to be pigeon-toed? Is it a quirky charm, a minor developmental hiccup, or a cause for genuine alarm?
To truly understand this phenomenon, we must embark on a journey – a story woven through the intricate landscape of human anatomy, the marvel of childhood development, the shifting sands of medical understanding, and the often-unspoken anxieties of parenthood. It’s a tale that begins not with a diagnosis, but with the very first stirrings of life, deep within the womb, and continues through the joyous, sometimes clumsy, process of learning to navigate the world on two feet.
Chapter 1: The Blueprint of Movement – What Pigeon-Toed Truly Means
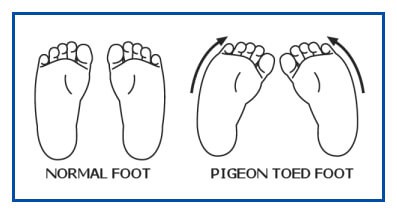
Imagine a bustling playground, a kaleidoscope of motion. Among the children chasing a ball, one little girl, let’s call her Elara, runs with an unmistakable inward turn of her feet. Her parents, watching from a bench, exchange a glance – a familiar mixture of love and subtle worry. "Pigeon-toed," one might murmur, a shorthand for what clinicians refer to as "in-toeing."
But Elara’s feet, while appearing to point inwards, are often just the visible manifestation of a twist originating much higher up the kinetic chain. The term "pigeon-toed" is a broad descriptor, a colloquial umbrella sheltering a few distinct anatomical realities. For our knowledgeable audience, it’s crucial to understand these underlying mechanics, as they dictate the course of observation and, in rare cases, intervention.
At its core, in-toeing describes a condition where the feet point towards each other rather than straight ahead when walking or standing. This inward orientation can stem from three primary areas of the lower limb, each with its own story and developmental trajectory:
-
Metatarsus Adductus (MTA): The Forefoot’s Gentle Curve
- This is often the earliest form of in-toeing to manifest, sometimes even visible at birth. Imagine Elara as a newborn, her tiny feet still bearing the imprint of her cozy, confined existence in the womb. Metatarsus adductus is characterized by the forefoot (the front part of the foot, including the toes) curving inward relative to the heel. It’s as if the foot has taken on a subtle C-shape.
- The Story of MTA: During fetal development, space can be tight. The baby’s feet might be held in a position that encourages this inward curvature. It’s akin to sleeping in a cramped position; once you stretch out, the stiffness resolves. For many infants, MTA is a flexible condition, meaning the foot can be gently straightened by hand. This flexibility is a good prognostic sign, suggesting it will likely resolve on its own as the baby grows and has more room to move and stretch. Less commonly, it can be rigid, indicating a more pronounced structural issue.
-
Internal Tibial Torsion (ITT): The Shin Bone’s Subtle Twist
- As Elara grows into a toddler, her parents might notice her entire lower leg seems to rotate inward. This is often the realm of internal tibial torsion, a twisting of the tibia, or shin bone. Picture the tibia as a long, cylindrical bone. In ITT, this cylinder has a subtle internal rotation along its length. When Elara stands, her kneecaps might point straight ahead, but her feet will still turn inwards because of this twist in her shin bones.
- The Story of ITT: Like MTA, ITT also has roots in the fetal position. Babies are often tucked into a ‘fetal position’ with their legs internally rotated for many months. This can lead to the bones and soft tissues adapting to this orientation. As children begin to stand and walk, the natural forces of weight-bearing and muscular development usually encourage the tibia to gradually untwist and align correctly. This process is fascinating; it’s the body’s ingenious way of correcting itself as it adapts to a new gravitational environment. ITT is most noticeable in toddlers and preschoolers, often peaking around 2-4 years of age.
-
Femoral Anteversion (FA): The Thigh Bone’s Internal Rotation
- Now, imagine Elara as a spirited 6-year-old. Her parents might observe that when she runs, not only do her feet turn in, but her knees also seem to angle inwards, sometimes appearing to "kiss" as she moves. This points to femoral anteversion, a twist in the femur, or thigh bone. In this case, the head and neck of the femur, which connect to the hip socket, are angled excessively forward relative to the shaft of the bone. This causes the entire leg, from the hip down, to rotate internally to allow the femoral head to sit comfortably in the hip socket.
- The Story of FA: This is arguably the most common cause of in-toeing in older children (typically 4-6 years old and often lasting until 8-10). It too is a remnant of fetal development. The unique "W-sitting" position, where a child sits on their bottom with knees bent and feet splayed out to the sides, is often associated with FA, though it doesn’t cause it. Rather, children with FA find this position comfortable because it allows their internally rotated hips to rest naturally. The natural resolution of FA is a slow, gradual process, often continuing throughout childhood, as the bone remodels and the soft tissues stretch and adapt.