In the annals of human health, few sagas are as compelling, as heart-wrenching, and ultimately, as triumphant as the story of HIV and AIDS. It is a narrative woven from threads of terror and despair, scientific brilliance and relentless dedication, social stigma and profound empathy. For a knowledgeable audience, the journey from an inevitable death sentence to a manageable chronic condition is not merely a collection of medical facts; it is a testament to human ingenuity and resilience, a story told in the language of molecular biology, clinical trials, and the unwavering spirit of those who live with the virus.
Chapter 1: The Shadow Emerges – The Early Days of Despair
The story begins in the early 1980s, cloaked in mystery and fear. A mysterious illness began to surface, characterized by a devastating collapse of the immune system, leaving individuals vulnerable to opportunistic infections and rare cancers. It was dubbed Acquired Immunodeficiency Syndrome (AIDS), and its cause, the Human Immunodeficiency Virus (HIV), was identified in 1983-84. The discovery was a watershed moment, but it offered little immediate solace. HIV was a cunning adversary, retrofitting the very machinery of human cells to replicate, primarily targeting CD4+ T-cells, the orchestrators of the immune response. As these vital cells dwindled, the body’s defenses crumbled, leading to the full spectrum of AIDS-defining illnesses.
In those initial years, an HIV diagnosis was a pronouncement of death. There were no treatments. Doctors could only manage the opportunistic infections, offering palliative care as the virus inexorably progressed. The average life expectancy after an AIDS diagnosis was tragically short, often measured in months. This era of profound despair, marked by rampant social stigma, fear, and a desperate search for answers, laid the grim foundation against which the monumental breakthroughs that followed would shine even brighter.
Chapter 2: Unveiling the Enemy’s Blueprint – HIV’s Life Cycle as a Strategic Map
To effectively combat HIV, scientists first had to understand its intricate modus operandi. The viral life cycle became the strategic map for drug development, revealing the vulnerabilities that could be exploited. For a knowledgeable audience, appreciating the sophistication of this cycle is key to understanding the elegance of modern treatments.
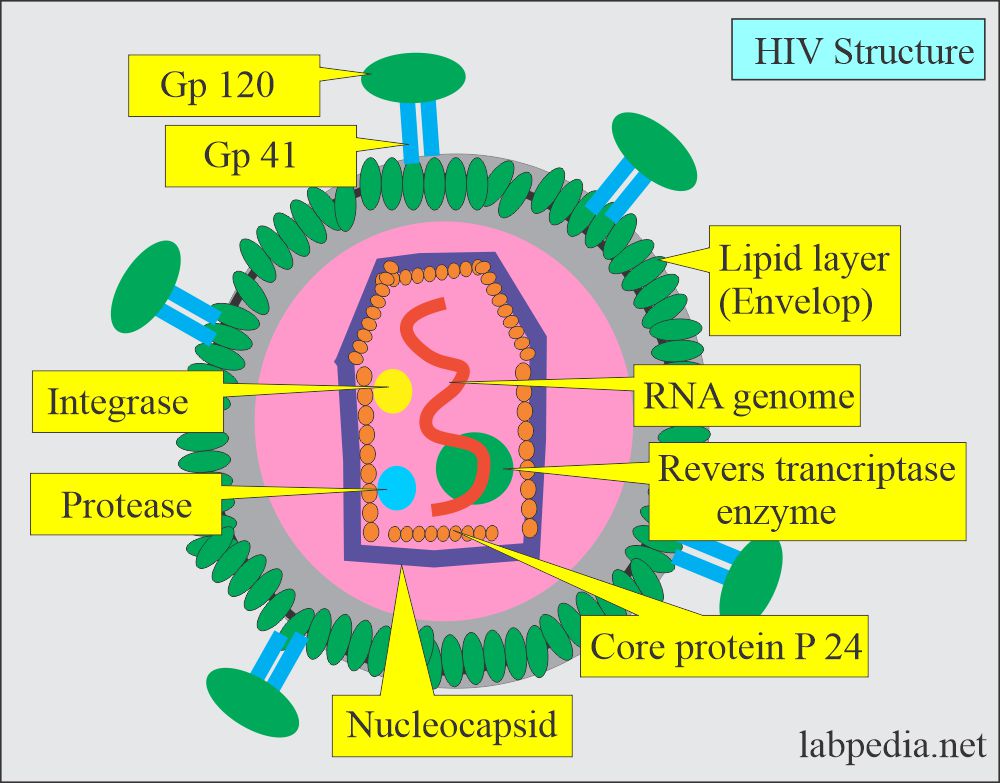
- Binding and Fusion: HIV’s outer envelope glycoprotein (gp120) first binds to the CD4 receptor on the host cell surface. This binding induces a conformational change, allowing gp120 to then bind to a co-receptor, typically CCR5 or CXCR4. This dual binding facilitates the fusion of the viral and host cell membranes, allowing the viral core to enter the cell.
- Reverse Transcription: Once inside, the viral enzyme Reverse Transcriptase (RT) converts the single-stranded viral RNA genome into a double-stranded DNA copy. This step is unique to retroviruses and is a prime target for early drugs.
- Integration: The newly synthesized viral DNA is then transported to the host cell nucleus, where another viral enzyme, Integrase, splices it into the host cell’s chromosomal DNA. From this point forward, the host cell is permanently infected and will serve as a factory for producing new viral particles. This integrated DNA is called a provirus.
- Transcription and Translation: The host cell’s machinery is hijacked to transcribe the proviral DNA back into viral RNA. Some of this RNA serves as the genetic material for new virions, while other RNA strands are translated into viral proteins.
- Assembly and Budding: Viral proteins and RNA molecules gather at the cell membrane, where they assemble into new, immature viral particles. These particles then bud off from the host cell, acquiring a piece of the host cell membrane as their outer envelope.
- Maturation: Finally, a viral enzyme called Protease cleaves long polyproteins into smaller, functional proteins. This maturation step is essential for the new virions to become infectious.
Each of these distinct stages represents a potential Achilles’ heel for the virus, a target for therapeutic intervention. Understanding this intricate dance was the first step in building an arsenal.
Chapter 3: The First Shots Fired – Early, Imperfect Weapons
The early 1980s were marked by an urgent, almost desperate, search for any drug that could slow the relentless march of the virus. The first major breakthrough came in 1987 with the approval of zidovudine (AZT), a nucleoside reverse transcriptase inhibitor (NRTI). AZT worked by mimicking the natural building blocks of DNA, but lacking the crucial 3′-hydroxyl group, it would terminate the growing viral DNA chain during reverse transcription, effectively halting the replication process.
The initial impact of AZT was profound. It offered a glimmer of hope, extending the lives of some patients and reducing opportunistic infections. However, its promise was quickly tempered by harsh realities. AZT was associated with significant side effects, including severe anemia and myopathy, making adherence difficult. More critically, HIV’s notorious ability to mutate rapidly meant that resistance to AZT often developed within months. Monotherapy, using a single drug, was ultimately a losing battle. The virus, a master of adaptation, could simply evolve around the solitary therapeutic pressure.
The realization that a single drug was insufficient paved the way for a paradigm shift. The fight against HIV required a multi-pronged assault, a strategy that would hit the virus at different points in its life cycle, making it far more challenging for resistance to emerge. This conceptual leap would transform the landscape of HIV treatment forever.
Chapter 4: The Arsenal Assembled – The Rise of Highly Active Antiretroviral Therapy (HAART)
The mid-1990s witnessed the true revolution in HIV treatment with the advent of Highly Active Antiretroviral Therapy (HAART), now more commonly referred to simply as Antiretroviral Therapy (ART). The strategy was elegantly simple: combine at least three different antiretroviral drugs from at least two different classes, each targeting a distinct stage of the HIV life cycle. This multi-pronged attack significantly reduced viral load (the amount of HIV in the blood) and allowed CD4+ cell counts to rebound, restoring immune function.
The impact of ART was nothing short of miraculous. From a death sentence, HIV became a manageable chronic condition. Hospitalizations plummeted, opportunistic infections became rare, and life expectancy soared. The "AIDS wards" that had been filled with terminally ill patients emptied, replaced by clinics focused on long-term management. This was the true turning point in the story, transforming despair into durable hope.
Modern ART regimens typically involve a backbone of two NRTIs combined with a third active agent from another class. Let’s delve into the major classes that form this powerful arsenal:
4.1. Nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NRTIs/NtRTIs)
These were the first class of drugs discovered and remain the cornerstone of most ART regimens. They are prodrugs that get phosphorylated inside the cell to become active. Like AZT, they mimic natural nucleosides/nucleotides and get incorporated into the growing viral DNA chain by reverse transcriptase, causing chain termination.
-
Key Agents:




