The human body is a symphony of subtle signals, a finely tuned instrument that, for most of our lives, we take for granted. We learn its basic melodies – hunger pangs, the ache of a tired muscle, the sting of a fresh cut. But there are discordant notes, faint whispers of discord that, if unheard or misunderstood, can lead to a profound and life-altering silence. For me, these were the early symptoms of HIV, a language I desperately wish I had understood sooner. This isn’t just an article; it’s a confession, a narrative woven from the threads of hindsight and the profound lessons learned after a diagnosis that irrevocably reshaped my understanding of health, vulnerability, and the deceptive nature of the human body.
My audience is knowledgeable, conversant with the medical lexicon and the broad strokes of HIV/AIDS. Therefore, I won’t dwell on basic definitions, but rather on the insidious nuances, the psychological toll, and the critical importance of interpreting those early, often dismissed, bodily pleas. This is the story of what I wish I knew, a story of symptoms that masqueraded as mundane, an enemy that hid in plain sight, and the stark clarity that only comes with a definitive diagnosis.
The Whispers Before the Storm: Acute Retroviral Syndrome (ARS) – What I Missed
Looking back, the first chapter of my story began with a subtle disquiet. Not a dramatic collapse, but a series of seemingly unrelated incidents, each easily rationalized away by the relentless pace of modern life. This period, now identified as Acute Retroviral Syndrome (ARS), is the body’s initial, often robust, response to the viral invasion. It typically occurs within 2 to 4 weeks after infection, a critical window of opportunity that I, like countless others, completely missed.
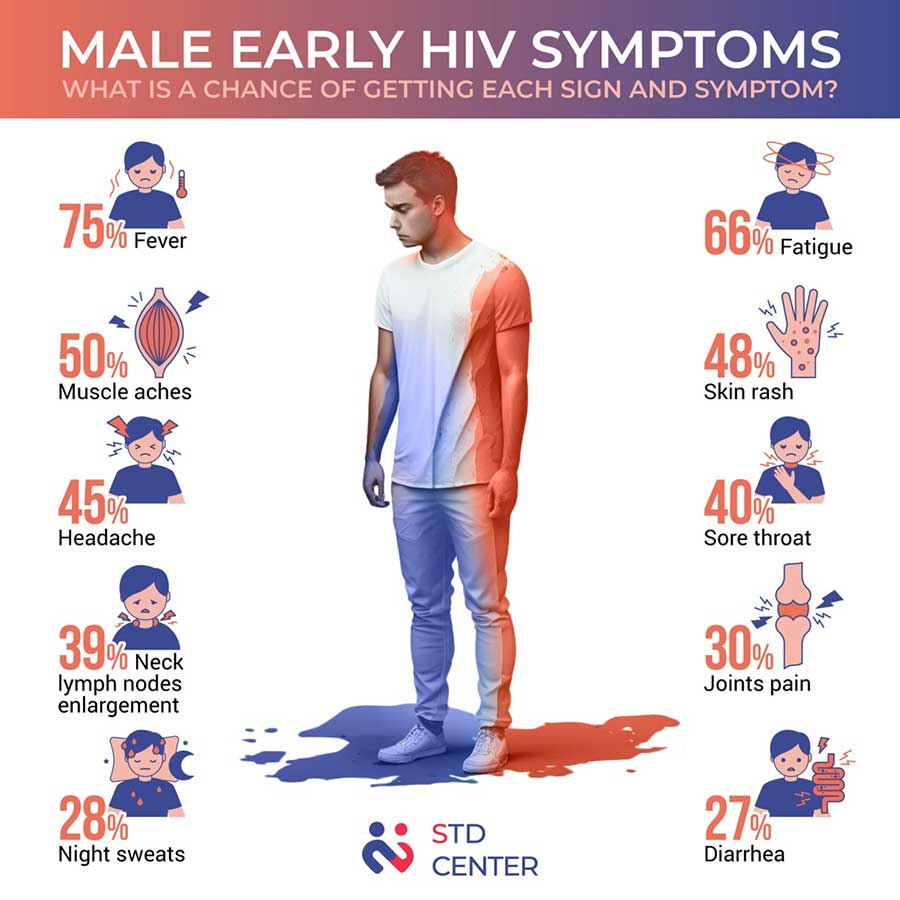
The classic descriptions of ARS often liken it to a severe flu, and that’s precisely how I dismissed it. It started with a persistent, low-grade fever that lingered for days, occasionally spiking higher in the evenings. I attributed it to stress, to a particularly demanding project at work, or perhaps to a common cold making its rounds. Fever is so ubiquitous, so unremarkable in its commonality, that it rarely triggers alarm bells unless accompanied by truly debilitating symptoms. Mine wasn’t debilitating; it was simply there, a simmering internal warmth I tried to ignore.
Then came the fatigue. Not just tiredness, but a profound, bone-deep exhaustion that no amount of sleep seemed to alleviate. It felt as though my energy reserves had been siphoned off, leaving me heavy-limbed and mentally foggy. I’d nod off during movies, struggle to concentrate during meetings, and find myself staring blankly at walls, devoid of motivation. My explanation? Burnout. Everyone talks about burnout, especially in my profession. It became my convenient scapegoat, a blanket diagnosis I wrapped myself in, unwilling to probe deeper.
A sore throat followed, an irritating scratchiness that made swallowing uncomfortable but never escalated to the debilitating pain of strep. I gargled with salt water, drank herbal teas, and blamed the dry office air. Simultaneously, my lymph nodes became noticeably swollen. I recall idly touching the tender, slightly enlarged nodes in my neck and armpits. My doctor, during a routine check-up for something else entirely, felt them and remarked, "Looks like you’re fighting something off, maybe a virus." That was enough for me. The medical professional had confirmed my own self-diagnosis: a generic viral infection. The knowledge that swollen lymph nodes are a hallmark of ARS, a sign of the immune system’s desperate initial battle, was completely absent from my understanding.
Perhaps the most distinctive, yet equally dismissed, symptom was a peculiar rash. It wasn’t itchy, nor did it blister like chickenpox. It was a maculopapular eruption, a scattering of small, flat, reddish spots and slightly raised bumps, primarily on my torso, face, and palms. It appeared suddenly, lingered for about a week, and then faded as mysteriously as it arrived. I remember looking at it in the mirror, puzzled. Was it an allergic reaction to a new detergent? Heat rash? Stress hives? I tried an antihistamine, which did nothing, and then simply waited for it to disappear, which it did. The idea that this non-specific rash could be a direct manifestation of seroconversion, the body reacting to the overwhelming influx of HIV, was a concept utterly foreign to my pre-diagnosis self.
Other symptoms surfaced: muscle aches (myalgia) and joint pain (arthralgia) that I attributed to a new workout routine, despite their unusual persistence. Headaches that were more frequent and intense than my usual tension headaches, prompting me to reach for ibuprofen more often. Occasional nausea and diarrhea, easily blamed on a dodgy takeaway meal or general stomach upset. Each symptom, in isolation, was so common, so readily explained by everyday occurrences, that their collective appearance failed to trigger the alarm bells that, in retrospect, should have been deafening.
What I wish I knew then was that the confluence of these symptoms, even if mild, within a few weeks of a potential exposure, should have been a screaming red flag. I wish I had known that the body’s immune response to HIV is often a systemic upheaval, not just a localized sniffle. I wish I had known to ask my doctor, explicitly, about HIV testing, rather than accepting a vague diagnosis of "viral infection." The opportunity for early diagnosis, for understanding the enemy while it was still establishing its foothold, slipped through my fingers like sand.
The Silent Siege: Clinical Latency and the Illusion of Health
After the initial flurry of ARS symptoms subsided, a deceptive calm descended. This is the stage known as clinical latency, or the asymptomatic stage. For years, I felt perfectly fine, even robust. My energy returned, my fevers vanished, and the rashes were long forgotten. This period can last for many years, even a decade or more, depending on the individual and the viral strain. It’s a period of profound irony: the person feels healthy, often healthier than they’ve ever been, while internally, a silent, relentless war rages on. The virus is actively replicating, gradually eroding the immune system, specifically the CD4+ T-cells, the critical orchestrators of the body’s defense.
This illusion of health is perhaps the most dangerous aspect of HIV. It breeds complacency, reinforces the belief that "nothing is wrong," and pushes the idea of testing further and further down the priority list. I continued to live my life, pursuing my career, enjoying social activities, and engaging in relationships, all while unknowingly harboring a pathogen that was systematically dismantling my protective barriers.
I recall moments of fleeting concern, usually after a casual encounter with an article or news report about HIV. A flicker of anxiety would spark, quickly extinguished by the overwhelming evidence of my apparent well-being. "I feel great," I’d tell myself. "It couldn’t be me." This self-deception was powerful, fueled by a combination of fear, ignorance, and the absence of any overt physical signs. What I wish I knew was that feeling "fine" after a potential exposure is not a guarantee of health; it is often the most treacherous phase of the infection, a calm before the storm of immune compromise. I wish I had understood that the absence of symptoms is not the absence of disease, and that the only way to truly know your status is to test.
The Alarms That Were Muted: Subtle Persistent Symptoms
Even during the prolonged period of clinical latency, my body was not entirely silent. There were ongoing, often subtle, persistent symptoms that, in hindsight, were clear indicators of a compromised immune system. These weren’t the acute, dramatic flares of ARS, but rather chronic, low-grade issues that became part of my "normal."
One of the most enduring symptoms was persistent generalized lymphadenopathy (PGL). My lymph nodes, particularly in my neck, armpits, and groin, remained subtly swollen and occasionally tender. I grew accustomed to them, even learned to ignore them. I’d occasionally ask a doctor about them during a physical, and the response was invariably, "Some people just have more prominent lymph nodes," or "It’s probably just benign reactive hyperplasia." These reassurances, while perhaps medically plausible in other contexts, were dangerously misleading in mine. What I wish I knew was that persistent, unexplained lymphadenopathy, especially if it affects multiple sites, is a significant red flag for HIV and other chronic infections. It’s the immune system perpetually engaged in battle, even when the rest of the body seems calm.
Then there was the chronic fatigue, which returned periodically, albeit less acutely than during ARS. It wasn’t the "I need a nap" kind of tired; it was a pervasive weariness that impacted my cognitive function, making it harder to focus, to recall information, and to sustain mental effort. I attributed it to aging, to poor sleep hygiene, to the general stress of modern life. I invested in better mattresses, tried various relaxation techniques, and consumed copious amounts of coffee, all to no avail. What I wish I knew was that chronic fatigue, unexplained and unrelenting, is a common symptom of advancing HIV infection, a sign that the body is diverting immense resources to fight the virus, leaving little for daily living.
Skin issues became a recurring nuisance. I developed persistent fungal infections, particularly oral thrush (candidiasis), which manifested as white patches on my tongue and inner cheeks. I dismissed it as a minor imbalance, a side effect of antibiotics I might have taken for something else, or simply "bad breath." I tried over-the-counter remedies, which offered temporary relief, but the underlying susceptibility remained. Athlete’s foot and jock itch became more frequent and harder to clear. Seborrheic dermatitis, characterized by flaky, red skin patches on my scalp and face, also worsened. These weren’t life-threatening, but they were persistent, irritating, and, in retrospect, screaming indicators of an immune system losing its grip. What I wish I knew was that recurrent or persistent fungal infections, especially oral thrush in an otherwise healthy adult, are a classic opportunistic infection in HIV, a canary in the coal mine signaling immune suppression.
Recurrent infections also plagued me. I seemed to catch every cold and flu that went around, and they lingered longer than they should have. Sinus infections became a regular occurrence, requiring multiple rounds of antibiotics. I’d joke about having a "weak immune system," never once considering why it might be weak. These weren’t severe, life-threatening infections, but they were more frequent, more tenacious, and less responsive to standard treatments than they should have been for a seemingly healthy individual. What I wish I knew was that an increased susceptibility to common infections, and their prolonged course, is a direct consequence of a compromised immune system struggling to cope with the viral load.
Weight loss, too, became a subtle companion. Not dramatic, emaciating weight loss, but a gradual, unexplained shedding of a few pounds over months. I initially welcomed it, attributing it to a slightly healthier diet or increased physical activity. But it continued, slowly, without conscious effort or significant dietary changes. I looked leaner, perhaps, but also a bit drawn. What I wish I knew was that unexplained weight loss, even if gradual, can be a symptom of chronic inflammation and metabolic changes induced by HIV, signaling the body’s increasing struggle to maintain its equilibrium.
Finally, night sweats. These were not the occasional mild perspiration of a warm night, but drenching sweats that would wake me, requiring me to change clothes or even sheets. I dismissed them as hormonal fluctuations, or perhaps just being a "warm sleeper." They were intermittent, making them easy to disregard, but their intensity was unusual. What I wish I knew was that drenching night sweats, unexplained by environmental factors or other obvious causes, are another classic, though non-specific, symptom of chronic infections, including HIV, indicating a heightened metabolic state as the body fights a persistent pathogen.
Each of these symptoms, in isolation, could be explained away. But their cumulative presence, their persistence, and their subtle deviation from my body’s baseline health should have prompted a deeper inquiry. The narrative I constructed for myself – "stress," "aging," "just a bug going around" – was a protective shield against a truth I wasn’t ready to confront.
The Unveiling: The Diagnosis and Retrospective Clarity
The moment of diagnosis, when it finally arrived, was a jarring intrusion into my carefully constructed illusion of health. It wasn’t triggered by a dramatic collapse, but by a routine medical check-up where my doctor, noticing the persistent lymphadenopathy and my recurring "minor" infections, suggested a comprehensive panel of tests, including HIV. The shock, the denial, the crushing weight of that conversation are memories etched permanently into my psyche.
But in the wake of the initial devastation came a profound, almost terrifying, clarity. Suddenly, all those disparate, dismissed symptoms clicked into place, forming a coherent and chilling narrative. The fever, the rash, the fatigue of ARS – they weren’t just a "bad flu"; they were my body screaming for help. The persistent lymph nodes, the recurrent thrush, the chronic fatigue, the night sweats – they weren’t just the quirks of my physiology; they were the slow, insidious manifestations of a virus relentlessly attacking my immune system.
It was a painful re-evaluation of my own body, a realization that I had been living in a state of self-deception, interpreting every signal through a lens of denial. I felt a profound sense of regret, not just for the missed opportunity of early treatment, but for the fundamental failure to listen to my own body, to trust its whispers, even when they were inconvenient or frightening.
The diagnosis brought with it a different kind of symptom management. No longer was I guessing; I was informed. The journey shifted from deciphering vague signals to actively monitoring viral load, CD4 counts, and engaging with antiretroviral therapy (ART). The symptoms I now experienced were often related to the initiation of ART (e.g., initial side effects, or Immune Reconstitution Inflammatory Syndrome – IRIS) or the long-term management of HIV, such as neuropathies, lipodystrophy, or cognitive changes, all of which are managed under the vigilant guidance of a specialized medical team. The difference was agency, knowledge, and proactive treatment.