The story of HIV is a testament to humanity’s capacity for both vulnerability and resilience. It is a narrative woven from threads of fear, scientific brilliance, social struggle, and ultimately, a profound understanding of a microscopic adversary. To truly grasp "What You Need To Know About HIV Causes," we must embark on a journey that transcends mere lists of risk factors, delving into the historical context, the intricate biology of the virus, and the complex interplay of human behaviors and societal structures that have shaped its global trajectory. This isn’t just about what causes infection; it’s about how we came to understand it, and what that understanding means for our present and future.
Chapter 1: The Shadow Emerges – Observing a Mystery
The early 1980s were marked by a disquieting medical enigma. Clinicians in major cities, particularly New York and Los Angeles, began reporting clusters of unusual diseases among young, previously healthy men. These were conditions rarely seen outside of severely immunocompromised individuals: Kaposi’s Sarcoma (a rare cancer), Pneumocystis Pneumonia (PCP), and other opportunistic infections. Initially dubbed "Gay-Related Immune Deficiency" (GRID), the scope of the problem soon broadened. Hemophiliacs receiving blood transfusions, intravenous drug users, and Haitian immigrants also began falling ill with similar, inexplicable immune collapses. A chilling pattern was forming, hinting at something far more sinister than a mere lifestyle-related illness.
The initial confusion was profound. Without a known pathogen, theories abounded, ranging from recreational drug use (specifically "poppers") to sexually transmitted infections (STIs) overwhelming the immune system, or even environmental toxins. Yet, epidemiologists, the disease detectives, quickly began piecing together crucial clues. The disease, whatever its cause, appeared to be transmissible. It clustered within specific populations, but more importantly, it spread through specific routes: sexual contact, blood transfusions, and shared needles. This pointed strongly towards an infectious agent, likely a virus, capable of being passed from person to person. The medical community began referring to the condition as Acquired Immunodeficiency Syndrome, or AIDS, a name that captured the essence of the immune system’s catastrophic failure.
The "4-H Club" – homosexuals, hemophiliacs, heroin users, and Haitians – became a shorthand for the initial risk groups. While later understood as an oversimplification and often stigmatizing, this early categorization was critical in guiding research. It suggested that the agent was present in bodily fluids – semen, blood – and could cross mucous membranes or be directly injected into the bloodstream. The narrative of "Patient Zero," Gaetan Dugas, a Canadian flight attendant, further solidified the idea of a sexually transmissible agent, although his role was later re-evaluated and largely debunked as the sole origin point. What was clear was that a silent, unseen enemy was spreading, and its true nature remained shrouded in terrifying mystery.
Chapter 2: The Invisible Enemy Revealed – Unmasking the Virus
The race to identify the causative agent of AIDS was one of the most intense scientific pursuits of the 20th century. Two prominent research teams, one led by Luc Montagnier at the Pasteur Institute in France and the other by Robert Gallo at the National Cancer Institute in the United States, were at the forefront. In 1983, Montagnier’s team announced the isolation of a novel retrovirus from a patient with lymphadenopathy, which they named Lymphadenopathy-Associated Virus (LAV). A year later, Gallo’s group reported the isolation of a virus from AIDS patients, which they called Human T-lymphotropic Virus Type III (HTLV-III). Despite an initial controversy over priority and patent rights, it was eventually confirmed that both groups had isolated the same virus. In 1986, the virus was officially named Human Immunodeficiency Virus, or HIV.
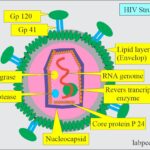
The identification of HIV was a monumental breakthrough. It wasn’t just any virus; it was a retrovirus. This distinction is critical to understanding its unique pathogenic mechanisms and the challenges in treating it. Unlike most viruses that use DNA to make RNA and then proteins, retroviruses have an RNA genome. Upon entering a host cell, they employ a specialized enzyme called reverse transcriptase to convert their RNA into DNA. This viral DNA is then integrated into the host cell’s own genetic material, becoming a provirus. This integration is a defining characteristic, meaning that once a cell is infected with HIV, it remains infected for its lifespan, serving as a permanent reservoir for the virus.
This integrated provirus can lie dormant for extended periods (latency), silently replicating along with the host cell’s own DNA. When activated, it hijacks the cell’s machinery to produce new viral particles. This insidious strategy allows HIV to evade the immune system for years, slowly eroding its defenses before the clinical symptoms of AIDS emerge. The discovery of HIV provided the missing piece of the puzzle, definitively linking the virus to the devastating immune collapse seen in AIDS patients. It satisfied Koch’s Postulates – the criteria for establishing a causal relationship between a microorganism and a disease – and transformed the global understanding of the epidemic.
Chapter 3: The Pathways of Transmission – How the Thread Spreads
With HIV identified, the focus shifted to understanding precisely how it spreads. The early epidemiological clues were largely confirmed and refined. HIV is transmitted through specific bodily fluids: blood, semen, pre-seminal fluid, rectal fluids, vaginal fluids, and breast milk. For transmission to occur, these fluids must come into contact with a mucous membrane (such as those found in the rectum, vagina, penis, or mouth), damaged tissue, or be directly injected into the bloodstream. It is crucial to emphasize that HIV is not transmitted through casual contact, air, water, or insects.
A. Sexual Transmission: The Primary Route
Globally, sexual contact remains the most common mode of HIV transmission. This occurs when HIV-containing bodily fluids from one partner come into contact with the mucous membranes or open sores of another partner during sexual activity.
- Anal Sex: This carries the highest risk among sexual acts for both receptive and insertive partners. The rectal lining is thin and delicate, making it more prone to micro-tears during intercourse, which can allow the virus to enter the bloodstream.
- Vaginal Sex: This is also a significant route of transmission. The vaginal lining can also sustain micro-abrasions, and the presence of cervical ectopy (a common condition where cells from inside the cervix are present on the outside) can increase vulnerability.
- Oral Sex: The risk of HIV transmission through oral sex is generally considered low, but not zero. It increases if there are open sores, bleeding gums, or other STIs present in the mouth or on the genitals.
- Factors Influencing Sexual Transmission: Several factors can increase the likelihood of transmission during sexual activity:
- Viral Load: The amount of HIV in an infected person’s bodily fluids. A higher viral load significantly increases the risk of transmission. Conversely, people on effective antiretroviral therapy (ART) who achieve and maintain an "undetectable viral load" cannot sexually transmit HIV (Undetectable = Untransmittable, or U=U).
- Presence of Other STIs: STIs like herpes, syphilis, gonorrhea, and chlamydia can cause inflammation, sores, or breaks in the skin/mucous membranes, creating entry points for HIV and increasing both susceptibility to and infectivity of HIV.
- Lack of Condom Use: Condoms, when used consistently and correctly, are highly effective in preventing HIV transmission.
- Circumcision: Male circumcision has been shown to reduce the risk of female-to-male HIV transmission by approximately 60%, as the foreskin contains cells (Langerhans cells) that are particularly vulnerable to HIV infection.
- Trauma: Any activity that causes tears or abrasions in the skin or mucous membranes can facilitate viral entry.
B. Blood-Borne Transmission: Direct Entry
Direct exposure to infected blood is a highly efficient means of HIV transmission.