The question of whether Bacterial Vaginosis (BV) should be classified as a Sexually Transmitted Infection (STI) is one that frequently surfaces in both clinical consultations and scientific discourse. It’s a question that, on the surface, seems straightforward, yet delves into the intricate biology of the human microbiome, the evolving understanding of disease transmission, and the very definition of an STI itself. For a condition as prevalent and impactful as BV, clarity on this classification is not merely academic; it has profound implications for diagnosis, treatment, prevention strategies, and public health messaging.
The prevailing scientific consensus, nuanced and complex as it is, leans away from categorizing BV as a classic STI in the same vein as chlamydia or gonorrhea. However, this stance is immediately followed by a crucial caveat: BV is undeniably and intimately associated with sexual activity, and its epidemiology, risk factors, and impact on sexual health bear striking resemblances to STIs. This article aims to unravel this complexity, exploring the scientific evidence, the ongoing debates, and the implications for our understanding of women’s reproductive health.
The Enigma of Bacterial Vaginosis: A Primer
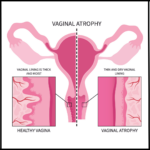
Before delving into the STI debate, it’s essential to understand what Bacterial Vaginosis truly is. BV is not an infection caused by a single, foreign pathogen, but rather a polymicrobial syndrome characterized by a disruption of the vaginal microbiome. In a healthy reproductive-aged woman, the vaginal ecosystem is typically dominated by Lactobacillus species, particularly Lactobacillus crispatus, which produce lactic acid, maintaining a low vaginal pH (around 3.8-4.5). This acidic environment acts as a natural defense mechanism, inhibiting the growth of most pathogenic bacteria.
In BV, this delicate balance is disrupted. There’s a dramatic decrease in beneficial Lactobacillus species and an overgrowth of a diverse array of anaerobic and facultative anaerobic bacteria. Key players in this shift include Gardnerella vaginalis, Prevotella species, Atopobium vaginae, Sneathia sanguinegens, Mobiluncus species, and various mycoplasmas. This microbial shift leads to an increase in vaginal pH (typically >4.5), the production of volatile amines (responsible for the characteristic "fishy" odor), and the formation of "clue cells" (vaginal epithelial cells covered in bacteria) visible under microscopy.
BV is the most common cause of vaginal discharge globally, affecting millions of women annually. While many women with BV are asymptomatic, others experience symptoms like malodorous discharge, itching, and burning. Beyond the discomfort, BV significantly increases the risk of acquiring and transmitting STIs, including HIV, herpes simplex virus (HSV), human papillomavirus (HPV), chlamydia, and gonorrhea. It’s also linked to serious reproductive health complications, such as pelvic inflammatory disease (PID), endometritis, infertility, and adverse pregnancy outcomes like preterm birth and miscarriage.
The Case Against BV as a "Classic" STI
The primary arguments against classifying BV as a traditional STI rest on several fundamental biological and epidemiological distinctions:
-
Polymicrobial Etiology vs. Single Pathogen:
A defining characteristic of classic STIs like gonorrhea (caused by Neisseria gonorrhoeae) or chlamydia (caused by Chlamydia trachomatis) is their causation by a single, specific, identifiable pathogen. BV, in contrast, is a dysbiosis, a shift in the balance of multiple bacterial species that are often endogenous to the vaginal flora, albeit in lower numbers in healthy states. While Gardnerella vaginalis is frequently implicated, it’s not the sole culprit, nor is its presence alone sufficient to diagnose BV. The absence of a single, transmissible etiological agent makes it challenging to fit BV into the classic STI paradigm. -
Endogenous Nature of BV-Associated Bacteria:
Many of the bacteria associated with BV, such as Gardnerella vaginalis and various anaerobes, can be found in small numbers in the vaginal microbiome of healthy, asymptomatic women. BV occurs when these opportunistic bacteria proliferate and outcompete the protective lactobacilli. This suggests an internal shift or susceptibility rather than the introduction of an entirely foreign, disease-causing organism. The analogy often used is that of an opportunistic infection, where the host’s defenses are compromised, allowing normal flora to become pathogenic. -
Occurrence in Sexually Inactive Individuals:
While rare, cases of BV have been documented in women who report no sexual activity, including virgins and pre-pubertal girls. This observation, though infrequent, directly challenges the notion of BV being exclusively transmitted through sexual contact. While alternative routes of transmission or predisposition are not fully understood in these cases, their existence suggests that sexual intercourse is not an absolute prerequisite for the development of BV. This stands in stark contrast to infections like gonorrhea, which are almost exclusively sexually acquired. -
Lack of Universal Transmissibility to Partners:
Unlike classic STIs where an infected individual can transmit the specific pathogen to their sexual partner, BV does not reliably transmit a "BV infection" to a male partner in the same manner. While men can harbor BV-associated bacteria on their penises, and this colonization might play a role in recurrence for their female partners (a point we will revisit), men do not typically develop a symptomatic condition analogous to BV. Similarly, female-to-female transmission, while observed, doesn’t always result in the same direct transfer of a defined "disease entity." -
High Recurrence Rates and Host Factors:
BV is notorious for its high recurrence rates, with up to 50-70% of women experiencing a recurrence within 6-12 months despite initial successful antibiotic treatment. This persistent challenge points towards underlying host factors, genetic predispositions, and lifestyle choices (including sexual practices) that make certain individuals more susceptible to dysbiosis, rather than simply reinfection by an external pathogen. Factors like vaginal douching, use of certain contraceptives, and even menstrual hygiene practices have been implicated in BV pathogenesis, highlighting the complex interplay of factors beyond direct sexual transmission.