The human immunodeficiency virus (HIV) is a master of disguise, an insidious enemy that often works in the shadows, particularly in women. For too long, the narrative around HIV focused on a male-centric presentation, overlooking the unique ways the virus manifests in the female body and the distinct societal, biological, and psychological factors that influence diagnosis and care. This article seeks to illuminate the common signs of HIV in women, not as a mere list of symptoms, but as a journey through the often-misunderstood landscape of a disease that whispers its presence before it roars. It is a story of vigilance, misdirection, and the profound importance of understanding one’s own body.
The Opening Act: Acute Seroconversion – A Fleeting Masquerade
The first act of HIV infection, known as acute seroconversion syndrome, is often the most deceptive. Occurring typically within 2-4 weeks after exposure, it’s the body’s initial, dramatic immunological response to the viral invasion. For many, it presents as a non-specific, flu-like illness that quickly fades, leaving no lasting impression of the profound battle that just took place beneath the surface. For women, this phase is particularly prone to misinterpretation, often dismissed as a common cold, seasonal flu, or even a stressful period.
Imagine Sarah, a vibrant 30-year-old, who suddenly feels utterly drained. A persistent headache throbs behind her eyes, her joints ache, and a low-grade fever hovers around 100°F. She might notice a faint, non-itchy rash on her torso, or swollen lymph nodes in her neck and armpits. These symptoms are her body’s desperate alarm bells, signalling a massive surge in viral load as HIV rapidly replicates. Yet, Sarah, like countless others, attributes it to overwork or a common viral infection. She might take some over-the-counter pain relievers, rest for a few days, and soon the symptoms vanish, leaving her none the wiser.
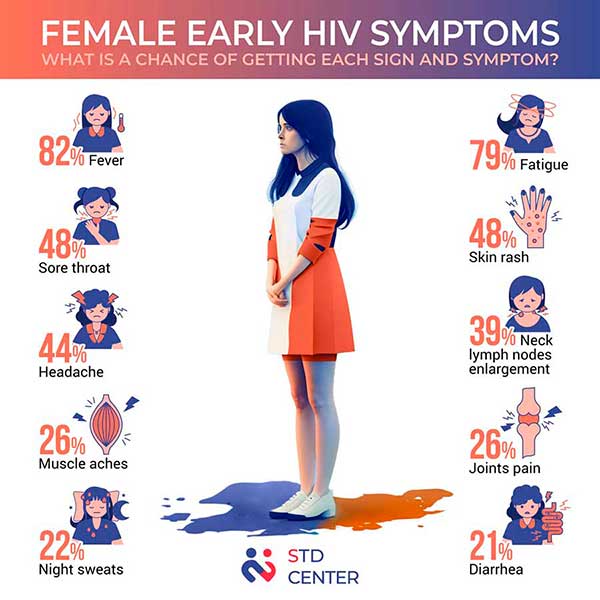
Key Acute Signs to Watch For:
- Fever: Often low-grade, persistent, and unexplained.
- Fatigue: Profound and debilitating, far beyond typical tiredness.
- Swollen Lymph Nodes (Lymphadenopathy): Commonly found in the neck, armpits, and groin, often tender.
- Rash: A maculopapular rash (flat, red spots sometimes raised) appearing on the torso, face, palms, or soles. It’s typically not itchy.
- Sore Throat (Pharyngitis): Often severe and accompanied by difficulty swallowing.
- Headache: Persistent and sometimes severe.
- Muscle and Joint Aches (Myalgia and Arthralgia): Widespread body aches.
- Nausea, Vomiting, Diarrhea: Gastrointestinal distress can occur.
- Oral Ulcers: Painful sores in the mouth, often mistaken for canker sores.
The crucial takeaway here is the non-specificity of these symptoms. They mimic so many benign conditions that even healthcare providers might not immediately consider HIV, especially without a direct prompt from the patient about potential exposure. For women, who are often socialized to prioritize others’ needs and downplay their own discomfort, this phase is often endured in silence, the brief storm passing without leaving a conscious trace of its true origin.
The Long Intermission: Clinical Latency – The Silent Saboteur
Following acute seroconversion, HIV enters its longest and arguably most dangerous phase: clinical latency. This is the period where the virus is actively replicating, silently attacking the immune system by destroying CD4+ T-lymphocytes, yet the individual often experiences no outward symptoms. This "asymptomatic" period can last for many years – typically 8 to 10 years, sometimes longer – during which the immune system slowly but steadily deteriorates.
This phase is the silent saboteur. A woman living with HIV in this stage might feel perfectly healthy, going about her daily life, unaware that a relentless battle is raging within her. This lack of overt symptoms contributes significantly to delayed diagnosis and, consequently, continued transmission. It’s during this extended intermission that the subtle, often overlooked, signs in women begin to emerge, if one knows where to look and how to interpret the body’s increasingly desperate pleas.
Subtle Clues During Latency (Often Overlooked or Misattributed):
While overtly asymptomatic, some women might experience very subtle, persistent issues that, in retrospect, serve as early indicators:
- Persistent Generalized Lymphadenopathy (PGL): Lymph nodes in two or more non-contiguous sites (other than the groin) that are swollen for more than three to six months. Unlike the acute phase, these nodes are often painless. This can be dismissed as benign.
- Mild, Recurrent Skin Issues: Unexplained, persistent dry skin, mild rashes that come and go, or skin infections that seem to take longer to heal.
- Unexplained Fatigue (Intermittent): Not as severe as in the acute phase, but a persistent feeling of being more tired than usual, even with adequate rest.
- Changes in Menstrual Cycle: While not directly HIV-specific, some women report subtle changes in their menstrual cycles, though these are often attributed to stress or hormonal fluctuations.
The real danger here lies in the normalcy. The absence of dramatic symptoms means HIV is rarely on the radar. This reinforces the critical importance of routine HIV testing, especially for women of reproductive age, regardless of perceived risk.