The pursuit of health and well-being often leads individuals down paths paved with hope and innovation. For millions living with Type 1 Diabetes (T1D), this journey is uniquely complex, marked by a daily tightrope walk of insulin management, blood glucose monitoring, and the ever-present shadow of complications. In recent years, a new beacon of hope has emerged for many: a class of powerful weight loss drugs, primarily GLP-1 receptor agonists and SGLT2 inhibitors, celebrated for their efficacy in shedding pounds and improving metabolic health in individuals with Type 2 Diabetes (T2D) and obesity.
But what happens when this compelling promise beckons those with Type 1 Diabetes, a condition fundamentally different from its Type 2 counterpart? The allure is undeniable. Many individuals with T1D grapple with weight gain, often a side effect of insulin therapy, alongside the inherent challenges of managing a chronic autoimmune disease. The prospect of an easier path to weight loss, potentially accompanied by improved glucose control, seems like a miracle. Yet, a growing chorus of endocrinologists and researchers is sounding a critical warning: for those with T1D, taking these drugs could come with a complex array of hidden risks, turning a perceived shortcut into a perilous detour. The story of these drugs in the T1D landscape is one of nuance, caution, and the profound importance of understanding fundamental physiological differences.
The Allure: Why T1D Patients Are Drawn to Weight Loss Medications
To understand the appeal, one must first appreciate the unique metabolic landscape of Type 1 Diabetes. Unlike T2D, where the body struggles with insulin resistance and often insufficient insulin production, T1D is characterized by the autoimmune destruction of pancreatic beta cells, leading to an absolute deficiency of insulin. This means survival is entirely dependent on exogenous insulin.
Insulin, while life-saving, is also an anabolic hormone. It promotes the storage of glucose as glycogen and fat. For many years, patients with T1D were advised to eat freely, as long as they covered it with insulin, leading to a higher prevalence of overweight and obesity compared to the general population. The fear of hypoglycemia often leads to overeating, and the constant need to manage glucose fluctuations can contribute to weight gain. Moreover, the very act of meticulously counting carbohydrates and calculating insulin doses can become mentally exhausting, sometimes leading to a less-than-optimal diet.
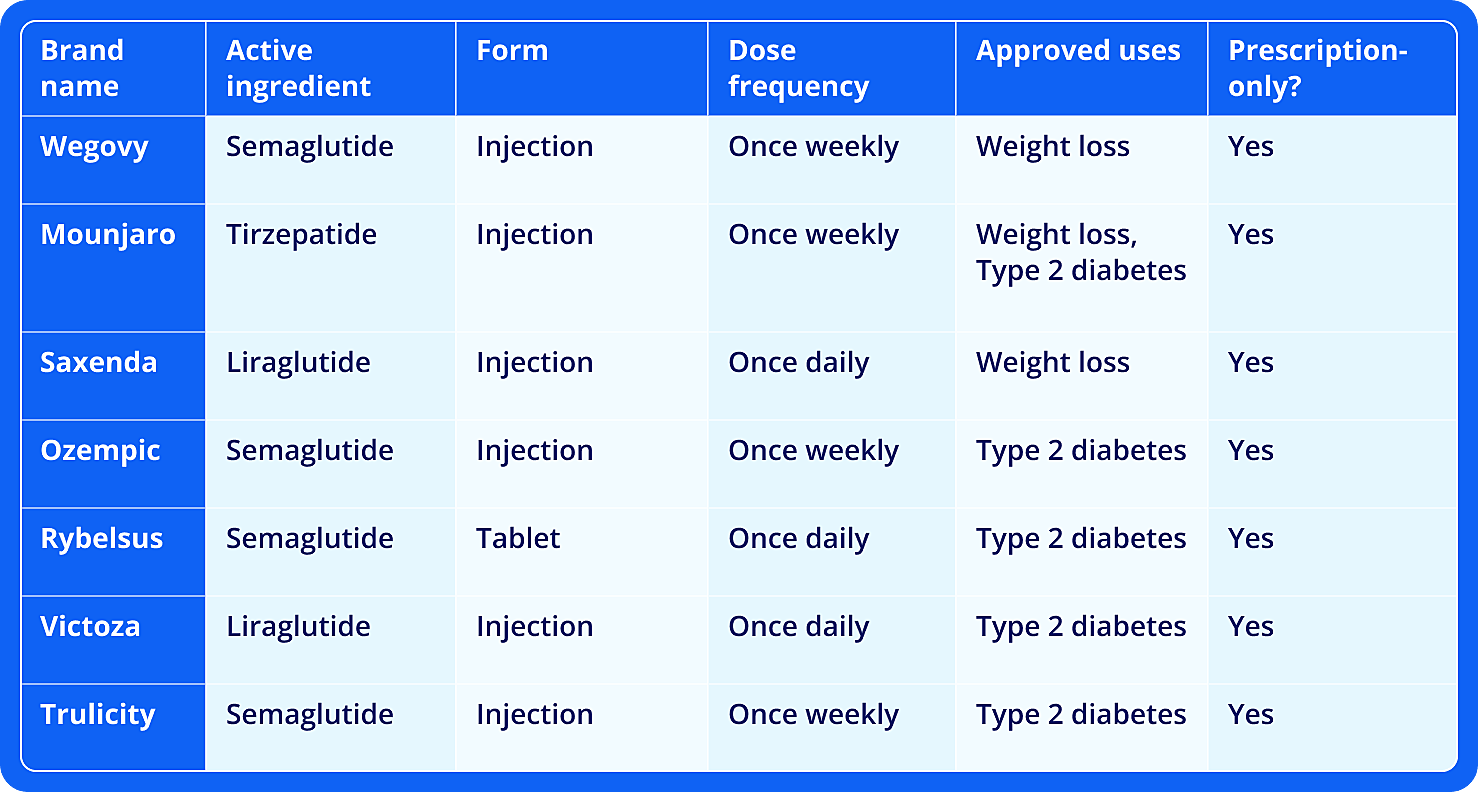
The advent of GLP-1 agonists like semaglutide (Ozempic, Wegovy) and liraglutide (Victoza, Saxenda), and the more recent tirzepatide (Mounjaro, Zepbound), has been revolutionary. These drugs work by mimicking incretin hormones, slowing gastric emptying, increasing satiety, and in T2D, stimulating glucose-dependent insulin secretion. The weight loss results are often dramatic, and many T1D patients, observing the success stories among their T2D peers, begin to wonder: could this be my answer too?
Adding to the complexity are SGLT2 inhibitors (e.g., empagliflozin, dapagliflozin, canagliflozin), which cause the kidneys to excrete more glucose in the urine. While initially developed for T2D, some were briefly approved for T1D (though often with strong caveats or subsequently withdrawn for this indication in some regions) due to their ability to lower blood sugar and offer cardiovascular and renal protective benefits. The weight loss associated with SGLT2 inhibitors, while less pronounced than GLP-1s, still contributes to their appeal.
The narrative of these drugs as a panacea for metabolic woes is powerful, creating a compelling siren song for individuals with T1D desperately seeking relief from the burdens of their condition, including the often-unspoken struggle with weight.
The Fundamental Difference: Why T1D Responds Differently
Herein lies the core of the hidden risks: the mechanisms of action for these drugs are designed for a body that still produces some insulin, however inefficiently. In T1D, that fundamental premise is broken.
GLP-1 Receptor Agonists: A Partial Symphony
GLP-1 receptor agonists primarily operate through several pathways:
- Delayed Gastric Emptying: This slows the rate at which food leaves the stomach, leading to a feeling of fullness and reducing post-meal glucose spikes. This effect does apply to T1D and is a significant contributor to weight loss and potentially smoother glucose curves.
- Increased Satiety: By acting on receptors in the brain, these drugs reduce appetite. This effect also applies to T1D.
- Suppression of Glucagon Secretion: Glucagon is a hormone that raises blood glucose. Reducing its secretion helps lower blood sugar. This effect also applies to T1D.
- Glucose-Dependent Insulin Secretion: This is the critical difference. In T2D, GLP-1 agonists stimulate the pancreas to release more insulin only when blood glucose is high. In T1D, the beta cells that produce insulin are destroyed. Therefore, this key mechanism, which helps prevent hypoglycemia in T2D and provides significant glucose-lowering benefit, is entirely absent.
This absence means that T1D patients taking GLP-1 agonists still rely entirely on injected insulin to prevent ketoacidosis and control blood glucose. The weight loss and appetite suppression are present, but the intrinsic safety net of glucose-dependent insulin release is gone. This fundamentally alters the risk profile.
SGLT2 Inhibitors: The Peril of Euglycemic DKA
SGLT2 inhibitors work by blocking the reabsorption of glucose in the kidneys, causing more glucose to be excreted in the urine. This lowers blood glucose levels. While this mechanism also applies to T1D, its interaction with insulin deficiency creates a unique and profoundly dangerous risk: euglycemic diabetic ketoacidosis (eDKA).
Diabetic ketoacidosis (DKA) is a life-threatening complication where the body, lacking sufficient insulin, starts breaking down fat for energy, producing acidic ketones. In typical DKA, blood glucose levels are very high. However, with SGLT2 inhibitors, the constant urinary excretion of glucose can lead to normal or only mildly elevated blood glucose levels, even as the body is producing dangerous levels of ketones.
Imagine a patient with T1D, diligently monitoring their blood sugar, who decides to take an SGLT2 inhibitor. Their blood sugar readings might look good, perhaps even slightly low, giving a false sense of security. Meanwhile, because the drug is forcing glucose out of the body, the cells are signaling an energy crisis. If insulin doses are reduced too much (perhaps in an attempt to avoid hypoglycemia, or simply because the blood sugars look good), the body enters a state of relative insulin deficiency. The liver, perceiving a lack of glucose, ramps up ketone production. The patient might feel tired, nauseous, or generally unwell, but without the classic high blood sugar alarms, they might delay seeking medical attention until DKA is severe. This "hidden" aspect – normal glucose levels masking a metabolic catastrophe – is what makes eDKA so insidious and life-threatening for T1D patients on SGLT2 inhibitors.
Unveiling the Hidden Risks: A Deeper Dive
The physiological differences described above translate into a range of specific and often hidden risks for T1D patients venturing into the realm of these weight loss drugs.
1. The Shadow of Hypoglycemia with GLP-1 Agonists
For a T1D patient, insulin dosing is a delicate dance. Add a GLP-1 agonist, which slows gastric emptying and suppresses appetite, and the choreography becomes exponentially more complex. If insulin doses aren’t meticulously adjusted downwards to account for reduced food intake and slower absorption, severe hypoglycemia can occur.
- Delayed Food Absorption: If a patient takes their pre-meal insulin and then experiences significantly delayed gastric emptying due to the GLP-1 agonist, the insulin might peak before the glucose from the meal has fully entered the bloodstream, leading to a dangerous low.



