The human body is an intricate symphony, a marvel of interconnected systems constantly striving for equilibrium. When an external threat breaches its defenses, this symphony can descend into discord, its notes becoming discordant cries for help. Few pathogens illustrate this profound disruption as acutely as the Human Immunodeficiency Virus (HIV). HIV is not a sudden, dramatic assailant; it is an insidious infiltrator, a master of disguise, whose true impact unfolds over years, telling a silent, yet devastating, story through the very fabric of the body it inhabits. To understand the signs and symptoms of HIV is to embark on a journey through the stages of a protracted battle, from the initial skirmishes to the full-blown siege, ultimately appreciating the remarkable transformation brought about by modern medicine.
For the knowledgeable audience, the narrative of HIV symptoms transcends a mere checklist of ailments. It is a chronicle of viral replication, immune erosion, and the body’s increasingly desperate attempts to compensate, adapt, and eventually, succumb without intervention. Each symptom, whether fleeting or persistent, serves as a poignant chapter in this unfolding story, providing clues to the virus’s progression and the depth of the immune compromise.
Chapter 1: The Initial Alarm – Acute Seroconversion Syndrome (The Body’s First, Often Misread, Cry)
The story of HIV’s symptomatic manifestation often begins subtly, approximately 2 to 4 weeks after initial exposure. This period, known as the acute seroconversion syndrome, or acute retroviral syndrome (ARS), represents the body’s first, vigorous, yet ultimately ineffective, attempt to mount an immune response against the rapidly replicating virus. During this phase, the viral load – the number of HIV particles in the blood – skyrockets, reaching astronomical levels, while CD4+ T-cells, the primary targets of HIV, experience a temporary but significant dip.
The symptoms of ARS are notoriously non-specific, earning it the moniker of "the worst flu ever." This lack of specificity is precisely why the initial alarm often goes unheeded, mistaken for a common viral infection, glandular fever, or even a severe cold. However, for those attuned to the nuances, the constellation and severity of these symptoms can hint at a more sinister underlying cause.
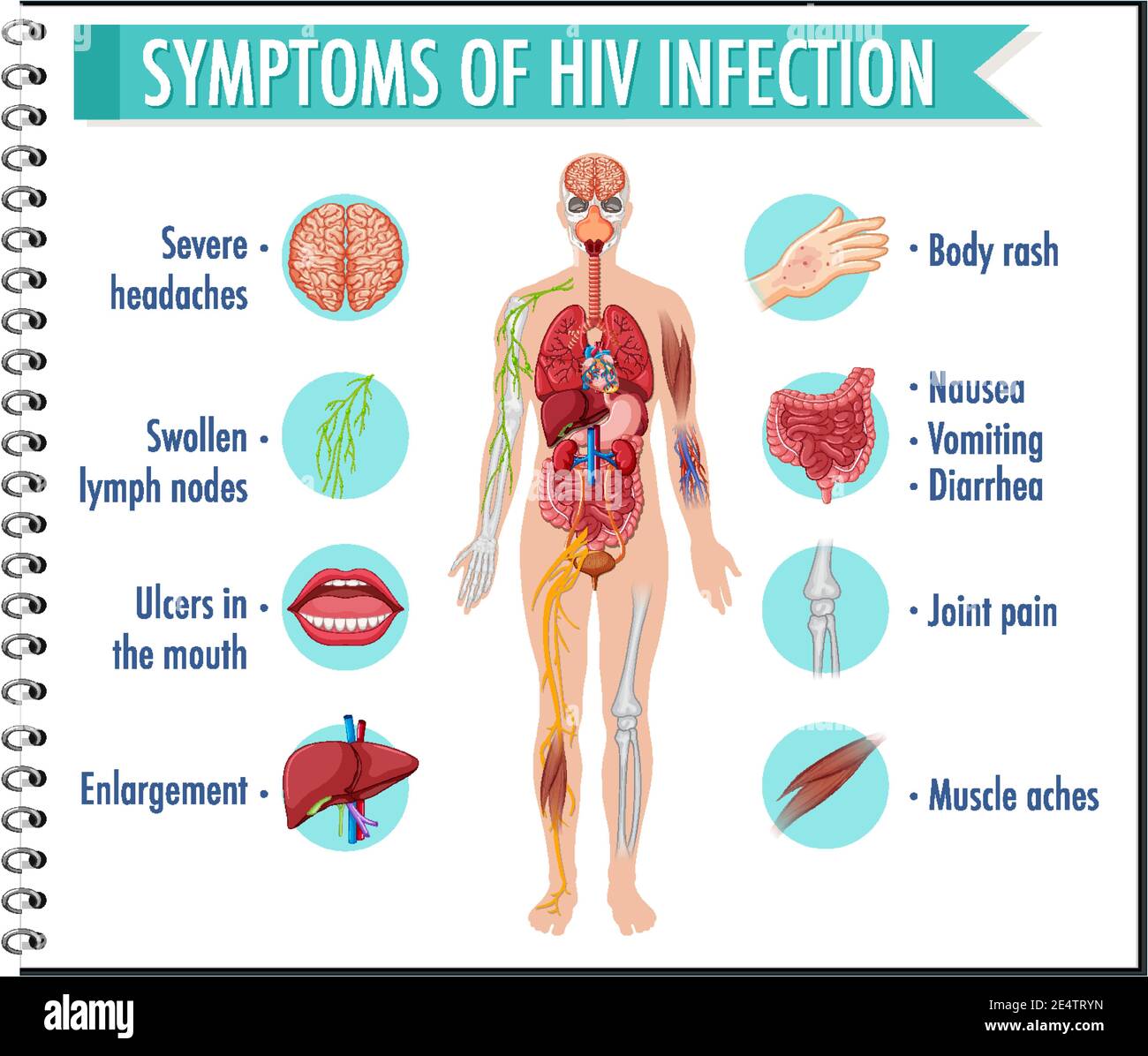
Key Symptoms of Acute Seroconversion Syndrome:
- Fever (96%): This is the most common symptom, often high-grade and persistent, reflecting the intense systemic inflammation triggered by widespread viral replication and the accompanying cytokine storm.
- Fatigue/Malaise (90%): Profound and debilitating tiredness, disproportionate to typical flu, can render individuals bedridden. This extreme fatigue is a direct result of the body’s energy expenditure in fighting the infection and the general systemic upset.
- Rash (70%): A characteristic maculopapular rash, typically non-itchy, often appears on the trunk, face, palms, and soles. Its appearance is due to the viral particles themselves or the immune reaction to them. It can be subtle or quite extensive, sometimes resembling measles or rubella.
- Lymphadenopathy (74%): Swollen, tender lymph nodes, particularly in the neck, armpits, and groin, are common. This is a direct sign of intense immune activity as the lymph nodes swell with activated lymphocytes attempting to contain the virus.
- Pharyngitis/Sore Throat (70%): A severe, often exudative sore throat, sometimes accompanied by painful swallowing (odynophagia), can be a prominent feature.
- Myalgia and Arthralgia (50%): Widespread muscle aches and joint pains, akin to a severe influenza infection, contribute significantly to the overall discomfort.
- Headache (32%): Can range from mild to severe, sometimes accompanied by photophobia or meningeal irritation, indicative of a possible aseptic meningitis due to viral invasion of the central nervous system.
- Gastrointestinal Symptoms (27%): Nausea, vomiting, and diarrhea, though less frequent than other symptoms, can also occur, adding to the systemic distress.
- Oral Ulcers/Aphthous Lesions (13%): Painful sores in the mouth or on the genitals can occasionally manifest, reflecting direct viral damage to mucosal tissues.
The acute phase is critical. Despite its often transient nature – symptoms typically resolve within a few weeks – it represents a period of extremely high infectivity due to the massive viral load. Early recognition and diagnosis during this window offer the best chance for timely intervention, preserving immune function and preventing onward transmission. However, the story here is often one of missed opportunities, as individuals and healthcare providers alike frequently attribute these symptoms to more benign causes.
Chapter 2: The Silent Siege – Clinical Latency (The Deceptive Calm)
As the acute seroconversion syndrome subsides, the story enters its most deceptive chapter: clinical latency. This phase, often lasting an average of 8 to 10 years without treatment, is characterized by a profound absence of overt symptoms. The body appears healthy, the individual feels well, and life seemingly returns to normal. Yet, beneath this veneer of wellness, a silent, relentless siege is underway.
During clinical latency, HIV continues its slow but steady assault on the immune system. While the viral load drops significantly from its acute phase peak, it remains detectable, and the virus continues to replicate, predominantly in lymphoid tissues. Crucially, CD4+ T-cells are progressively destroyed, albeit at a slower rate than in the acute phase. The immune system, a remarkable adaptive machine, compensates for this loss for a considerable time, producing new CD4+ cells to replace those destroyed. However, this regenerative capacity is finite. Eventually, the rate of destruction outpaces the rate of production, leading to a gradual, inexorable decline in CD4+ cell count.
The "story" of this phase is one of hidden erosion. The knowledgeable audience understands that "asymptomatic" does not mean "inactive." It signifies a period where the body’s robust compensatory mechanisms are still largely effective, masking the ongoing damage. Nevertheless, some subtle clues may emerge, foreshadowing the deeper immune compromise to come.
Subtle Manifestations During Clinical Latency:
- Persistent Generalized Lymphadenopathy (PGL): This is perhaps the most common and often the only physical sign during prolonged latency. PGL is defined as enlarged lymph nodes (greater than 1 cm in diameter) in two or more non-contiguous extra-inguinal sites, persisting for at least 3 to 6 months, in the absence of any other obvious cause. These nodes are usually non-tender, firm, and mobile. While not immediately threatening, PGL signifies ongoing viral replication and immune activation within the lymphoid tissues.
- Minor Mucocutaneous Manifestations: Occasionally, individuals may experience recurrent, mild skin conditions or oral lesions that, while not AIDS-defining, are more frequent or severe than in the general population. These might include:
- Seborrheic Dermatitis: More extensive or recalcitrant than usual.
- Fungal Nail Infections (Onychomycosis): More prevalent and harder to treat.