In the vast, intricate landscape of human health, there exist conditions that, while common, remain shrouded in a peculiar blend of misunderstanding, fear, and silence. Genital warts are undeniably one of them. They are more than just a dermatological manifestation; they are a story – a narrative woven from the microscopic dance of viruses, the complex mechanics of the human immune system, and the profound psychological and social ripples they cast upon individuals. To truly understand genital warts is to embark on a journey beyond the visible lesions, delving into the unseen architect behind them, the paths they traverse, and the resilience of those who encounter them.
Our audience here is not seeking a superficial overview but a comprehensive, nuanced exploration. We peel back the layers of stigma and misinformation, revealing the scientific intricacies, the human experience, and the pathways to management and prevention. This is the story of genital warts, told not as a medical bulletin, but as a narrative of a ubiquitous viral encounter.
Chapter 1: The Invisible Architect – Human Papillomavirus (HPV)
Every story has its protagonist, and in the saga of genital warts, that role is unequivocally played by the Human Papillomavirus, or HPV. Far from a singular entity, HPV is a sprawling family of over 200 distinct types, each a microscopic architect capable of influencing human cells in various ways. It’s crucial to understand this diversity, for it dictates the narrative’s direction.
Among this vast viral family, two distinct lineages emerge in our tale: the "low-risk" types and the "high-risk" types. It is predominantly the low-risk types – most notably HPV types 6 and 11 – that are the invisible architects of genital warts. These specific strains are experts at inducing benign cellular proliferation, leading to the characteristic wart formations. They are, importantly, rarely associated with cancer. Conversely, the high-risk types, such as HPV 16 and 18, are the notorious instigators of cellular changes that can, over time, progress to various cancers, including cervical, anal, oral, and other anogenital cancers. This fundamental distinction is paramount: genital warts, in and of themselves, are not cancerous, nor are they a direct precursor to cancer, although they share a common viral lineage with cancer-causing HPVs.
The journey of HPV into its human host is typically one of intimate, skin-to-skin contact. While often categorized under sexually transmitted infections (STIs), this label sometimes creates a misleading image of transmission requiring penetrative intercourse. In reality, HPV can be transmitted through any skin-to-skin contact in the genital area, including oral sex, manual-genital contact, and even instances where there is no explicit sexual penetration. The virus simply requires a micro-abrasion or break in the skin or mucous membrane to gain entry into the basal layer of epithelial cells, where it sets up residence.
Once the virus has gained entry, it begins its silent incubation. This phase is perhaps one of the most frustrating and bewildering aspects of HPV infection. The incubation period for genital warts can range from a few weeks to many months, and sometimes even years, after exposure. An individual might contract the virus from a partner, and the warts might not appear until long after that relationship has ended, or even after they have been with a new partner. This latency makes pinpointing the exact source of infection often impossible and can sow seeds of doubt and suspicion, further complicating the emotional landscape. The virus essentially lies dormant or replicates at a low level, undetected by the host’s immune system, waiting for an opportune moment to manifest.
The immune system, our body’s diligent sentinel, plays a pivotal role in this unfolding drama. For the vast majority of individuals who encounter HPV, their immune system successfully mounts a response, clears the virus, and prevents any visible manifestations. This silent clearance occurs in an estimated 90% of cases within two years. These individuals may never know they were infected. However, for a smaller percentage, the immune system might not be as effective, or the viral load might be higher, leading to persistent infection and, eventually, the emergence of warts. Factors like a weakened immune system (due to conditions like HIV/AIDS, organ transplantation, or certain medications), smoking, or concurrent infections can increase the likelihood of persistent infection and wart development. The immune system’s varying responses underscore the individuality of the HPV story, where exposure doesn’t automatically equate to visible disease.
Chapter 2: The Manifestation – What Are Genital Warts, Really?
After its silent incubation, the virus, if it persists, begins to sculpt its visible testament: the genital wart. For many, this is the first tangible sign of an invisible guest, and its appearance often initiates a cascade of emotions – confusion, fear, shame, and anxiety. To demystify them, we must first describe their physical presentation.
Genital warts typically present as small, flesh-colored, or slightly darker bumps. They can be singular or, more commonly, appear in clusters that might resemble miniature cauliflowers. Their texture can vary; some are smooth and dome-shaped (papular), others are flat, and some are distinctly stalk-like (pedunculated). They can be soft to the touch or slightly firmer, depending on their age and location.
The locations where these manifestations choose to appear are diverse, reflecting the areas of skin-to-skin contact. In males, they commonly appear on the penis (shaft, glans, foreskin), scrotum, around the anus, and in the perineal area. In females, they are frequently found on the vulva, within the vagina, on the cervix (though often asymptomatic here), around the anus, and in the perineum. Less commonly, but still possible, they can appear in the inner thighs or groin area, or even in the oral cavity if oral sex was involved in transmission. The varying topography of these anatomical sites influences how the warts look and behave. Warts in moist areas, like the vaginal canal, might be flatter and less visible, while those on dry skin, like the penile shaft, might be more pronounced.
For many, the warts themselves cause no physical discomfort. They are merely a visual presence. However, for others, symptoms can arise. These might include itching, which can be intense and irritating; burning sensations, particularly after urination or friction; a sense of discomfort or tenderness; and, in some cases, bleeding, especially if the warts are large, located in areas of friction, or traumatized during sex or hygiene practices. The psychological discomfort, however, often far outweighs the physical.
The emergence of genital warts often triggers a profound psychological impact. The knowledge of having an STI, even a common and benign one, can lead to feelings of shame, self-blame, and a damaged sense of self-worth. There’s an inherent fear of judgment from partners, friends, and even healthcare providers. Intimacy can become a source of anxiety, with individuals worrying about transmission, partner reaction, or simply the aesthetics of their own body. This emotional burden is a significant, often overlooked, chapter in the story of genital warts, underscoring the need for empathetic care and destigmatization.
It’s also vital to acknowledge that not every bump or lesion in the genital area is a wart. The body is a landscape of diverse dermatological features, and many benign conditions can mimic the appearance of warts, leading to unnecessary alarm. These include molluscum contagiosum (another viral infection causing small, dome-shaped lesions with a central dimple), skin tags, sebaceous cysts, Fordyce spots (visible sebaceous glands), and pearly penile papules (small, benign bumps around the corona of the glans penis). This differential diagnosis highlights the critical importance of professional medical evaluation; self-diagnosis, driven by fear or internet searches, often leads to misinterpretation and heightened anxiety.
Chapter 3: The Quest for Understanding – Diagnosis and Confirmation
The discovery of a new, unusual bump in an intimate area is often the catalyst for the "quest for understanding." This journey usually begins with self-examination, a partner’s observation, or sometimes, a serendipitous finding during a routine medical check-up. Regardless of the trigger, the next crucial step is seeking professional medical advice.
The healthcare provider acts as the guide in this quest, bringing expertise and an objective perspective. The diagnostic process for genital warts is primarily clinical, meaning it relies heavily on visual inspection. An experienced clinician can often identify genital warts based on their characteristic appearance, location, and typical morphology. They will conduct a thorough examination of the anogenital area, sometimes using a magnifying glass (colposcope or dermatoscope) to better visualize the lesions.
One common diagnostic tool sometimes employed is the acetic acid test, often referred to as the "white vinegar test." In this procedure, a dilute solution of acetic acid (the active ingredient in white vinegar) is applied to the suspected area. If HPV-infected cells are present, they may turn white after a few minutes, a phenomenon known as "acetowhitening." The acetic acid temporarily dehydrates the cells, making them appear opaque. While seemingly straightforward, this test has significant limitations. It is not specific to HPV; other benign conditions, such as inflammation, abrasions, or even thick skin, can also turn white, leading to false positives. Conversely, some warts may not acetowhiten, leading to false negatives. Therefore, the acetic acid test is rarely conclusive on its own and is generally used as an adjunct to visual inspection, if at all, to highlight subtle lesions. It should never be used for self-diagnosis, as it can cause irritation and lead to misinterpretation.
In cases where the diagnosis is uncertain, the warts have an atypical appearance, they are resistant to treatment, or there’s a concern about potential malignancy, a biopsy may be performed. This involves taking a small tissue sample from the wart, which is then sent to a pathology lab for microscopic examination. A pathologist can definitively confirm the presence of HPV-induced changes, rule out other conditions, and, importantly, confirm that the lesion is benign, offering immense reassurance.
It’s important to clarify the role of HPV DNA testing in the diagnosis of genital warts. While HPV is the causative agent, HPV DNA testing (like the tests used for cervical cancer screening) is generally not recommended for the routine diagnosis of genital warts. These tests are designed to detect the presence of specific high-risk HPV types in cervical cells to screen for cancer risk, not to identify the low-risk types that cause warts. Furthermore, a positive HPV test, particularly in the absence of visible warts, simply indicates the presence of the virus, which is extremely common and often asymptomatic. Its clinical utility for wart management is limited. The diagnosis of genital warts remains primarily a clinical one.
Beyond the physical examination and tests, the diagnostic journey also involves a crucial conversation. A knowledgeable and empathetic healthcare provider will not only diagnose the condition but also educate the individual about HPV, its transmission, treatment options, and the emotional impact. This conversation is vital for dispelling myths, addressing fears, and empowering the individual with accurate information, laying the groundwork for effective management and emotional well-being.
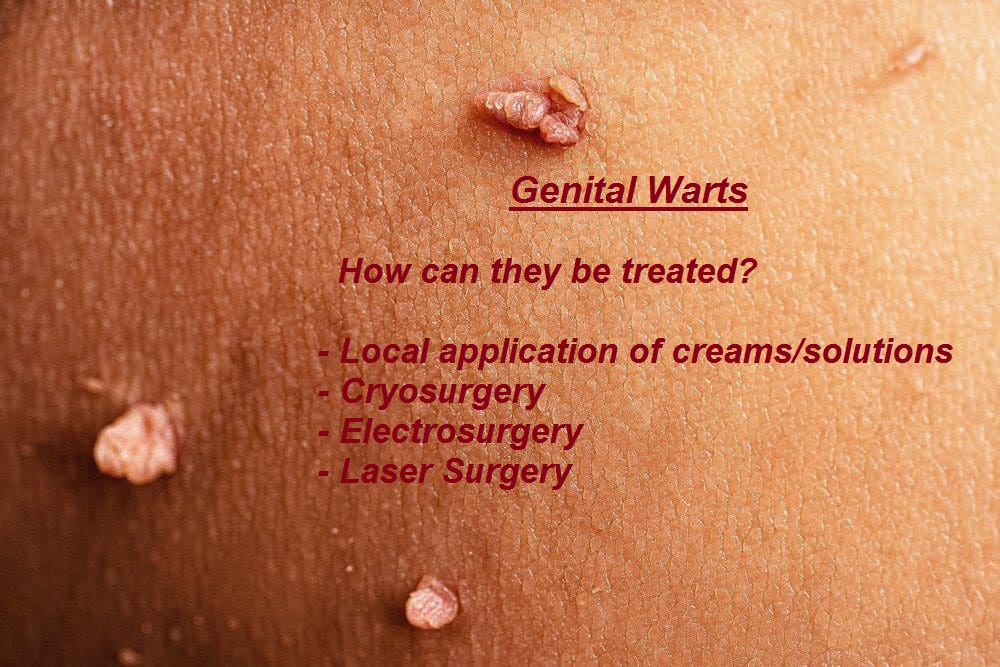
Chapter 4: The Path to Resolution – Treatment Options
Once the diagnosis of genital warts is confirmed, the story turns to resolution – the pursuit of eradicating the visible lesions. This chapter, however, carries a crucial caveat: while treatments can effectively remove the warts themselves, they do not cure the underlying HPV infection. The virus may remain dormant in the surrounding skin, which explains why warts can recur even after seemingly successful treatment. This distinction is vital for managing expectations and understanding the long-term journey with HPV.
Treatment approaches for genital warts fall into two main categories: patient-applied topical medications and provider-administered procedures. The choice of treatment depends on several factors, including the number, size, and location of the warts, patient preference, cost, potential side effects, and the clinician’s expertise.
Patient-Applied Therapies (The Home Front):
These treatments are prescribed by a healthcare provider but applied by the patient at home, offering convenience and privacy.
- Podofilox (Condylox): This is an antimitotic agent that works by disrupting cell division, effectively stopping the growth of the wart cells. It is typically applied twice daily for three days, followed by four days of no treatment, for up to four cycles. Common side effects include local skin irritation, redness, and erosion. It is not safe for use during pregnancy.



